A 1994 article in the New England Journal of Medicine (“Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation” by Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L.) effectively launched cartilage repair in the United States.
Getting Cartilage Repair Right – After 25 Years
8 min read Premium comments
#cartilagerepair#cartiheal#cartilagelesion#agilic
One year later Boston-based Genzyme Corporation took the autologous chondrocyte transplantation (ACI) technology described in the NEJM article and created a cartilage repair product and process named Carticel.
Two years after that, the FDA granted Genzyme a license for Carticel. It was the first time the FDA had licensed/approved or cleared a living cell technology for commercial sale.
Jump ahead 25 years, and after more than 1 million annual cartilage treatment procedures in the U.S., including 430,000 debridement procedures and 220,000 microfracture surgeries (source: SmartTRAK.net – Cartilage Replacement – U.S., January 3, 2019), cartilage repair remains more a hope than a standard of care.
Carticel along with another ACI treatment, MACI (autologous cultured chondrocytes on porcine collagen membrane), are the most popular cartilage repair technologies in the United States. Those treatments (along with a related technology for wound repair—Epicel) generate about $40-45 million in annual product sales.
Other cartilage repair products that were also developed include Zimmer’s DeNovo-NT, plug-type scaffolds for arthroscopic delivery like Dunlop Corp’s carbon fiber plug or Smith & Nephew’s True-Fit plug, Tigenex’s Chondromimetic implant and Histogenic’s NeoCart (collagen scaffold with autologous living cells).
Even so, within the overall market to treat deteriorating knees, cartilage repair product sales barely register.
In terms of dollars ($7 billion), knee replacement surgery is the principal treatment modality for patients suffering from end-stage osteoarthritis. Hospitals, physicians, suppliers and payers understand that that is the bread and butter of the industry.
A quick perusal of American Academy of Orthopaedic Surgeons’ (AAOS) clinical practice guidelines for osteoarthritis (OA) of the knee finds a whole range of pre-knee replacement therapies including NSAIDs, cortisone shots, platelet rich plasma injections and osteotomies.
But no technologies for cartilage repair or regeneration.
Sanofi, the company that came to own Carticel, Epicel and MACI sold that 230 employee business in 2014 for just $4.0 million (with a $2.5 million note) to Aastrom Biosciences, since renamed Vericel Corporation.
Cartilage repair, for sure, is not burdened by great expectations.
So, Why Are Cartilage Scientists Getting Excited?
Given that short history, why then are three of the top cartilage repair scientists in the world excited about a specific ongoing FDA cartilage repair clinical study which, in their own words, may be the most impactful new development in cartilage repair and, by extension, the $7 billion a year business of treating painful, impaired knees in, well, 25 years?
We’re referring to:
Elizaveta Kon, M.D., Ph.D.: Associated Professor of Humanitas University, Orthopaedic surgeon on Center of Functional and Biological Reconstruction of the knee, Humanitas Research Hospital, full professor of Orthopaedic Surgery on First Moscow State Medical University (Sechenov University), Moscow, Russia. 2nd Vice President of the International Cartilage Regeneration & Joint Preservation Society (ICRS), author of over 200 scientific articles in peer-reviewed journals and over 30 chapters in textbooks in orthopedic surgery, Associated Editor of International Orthopedics, Journal of Experimental Orthopedics and Joints.
Kenneth Zaslav, M.D.: Orthopedic surgeon with Ortho Virginia, one of the largest private Orthopedic multi-specialty groups in the U.S. Clinical Professor at the Department of Orthopaedic Surgery at Virginia Commonwealth University, immediate Past President of The International Cartilage Repair Society, visiting professor in medical schools in China, Chile, Mexico and Venezuela, Past President of Advanced Orthopaedics and board certified orthopedic surgeon in Virginia.
Peter Verdonk, M.D., Ph.D.: Specialist knee surgeon (Antwerp, Brussels, Ghent, Belgium) and researcher at the Antwerp University and the Monica Research Institute. Visiting surgeon at the Aspetar Hospital in Doha, Qatar and an attending surgeon and professor at the Antwerp University Hospital. His Ph.D. thesis was “The Human Meniscus: characterization, transplantation and tissue engineering.” He is author of more than 100 peer-reviewed papers and lectures internationally.
And the clinical study they are excited about is NOT about “stem cells,” PRP, autologous chondrocytes transplantation or even OATS (osteoarticular transfer system) or HA (hyaluronic acid). It’s about a novel implant that is in a paradigm shifting clinical study for the treatment of joint surface lesions, including, cartilage and osteochondral defects in both arthritic and non-arthritic joints. Extremely interesting.
Have You Ever Seen a Clinical Study Like This?
The study is the Agili-C study, sponsored by Israeli-U.S. based CartiHeal Ltd, and funded by Johnson & Johnson, Bioventus, Elron, Accelmed, Access Medical Ventures, aMoon and Peregrine Ventures.
The following table is a comparison of cartilage repair studies BEFORE Agili-C and then the first-of-its-kind Agili-C study – FDA sanctioned.
| BEFORE Agili-C | Agili-C[1] | |
| Age of Patients | Usually up to 55 | Up to 75 |
| Presence of Osteoarthritis | NO | Yes (mild-moderate) |
| Number of Lesions | 1-2 | Up to 3 |
| Type of Defects | Cartilage | Cartilage and ostoechondral |
| Concomitant Procedures | Not allowed | Allowed: meniscectomy and HTO |
| Total Defect Size: | 1-4 cm[2] (usually 2 cm2) | 1-7 cm2 |
| Previous Failed cartilage Treatment | Not allowed[3] | Allowed |
| Control / Comparator: | Microfracture[4] | Microfracture and debridement |
| Malalignment Exclusion? | Yes[5] | No (up to 8⁰) |
| Defect Location: | Single Condyle Only | 1 or 2 Condyles, Condyle & Trochlea, 2 Condyles & Trochlea |
The range of defects is large, just like a typical patient population in any orthopedic clinic.
The age range is huge (21-75 years).
The control arm is, effectively, the current common surgical standard of care, microfracture or debridement—not just microfracture.
The number of defects can be as many as three and malalignment is NOT an exclusion (up to 8°).
“The Agili-C trial is very close to real life,” Dr. Verdonk told OTW. “Randomization is versus current standard of care—either debridement or microfracture. Which is a major advantages of the Agili-C study.”
One of the effects of broad inclusion criteria is that the 250-patient study is enrolling notably quickly. Said Dr. Zaslav: “I’ve never seen a study enroll this fast. We’ve already got nearly 200 patients in about one and a half years, and we need 250 until our first Interim Analysis—which we should probably have before year end. The other studies it took four to five years to enroll this number of patients.”
Because the study includes patients with mild to moderate osteoarthritis and allows randomization against EITHER microfracture or debridement, enrollment has really popped.
The randomization allocation ratio is 2:1—for every two patients randomized to the implant, one is randomized to control.
It should be noted that as in previous studies, young patients with small, focal defects but no arthritis, are receiving microfracture. Older patients with large lesions and mild to moderate osteoarthritis are randomized against debridement (small focal defects with KL=0 cannot be treated with debridement).
Again, Dr. Zaslav: “A lot of people don’t want microfractures, so it’s hard to get enough patients in a study randomized to microfracture alone.”
Dr. Kon explains some of the etiology of this novel study design: “Many surgeons believe that microfracture should not be performed to treat large lesions and in presence of osteoarthritis. Performing microfracture in these patients may enhance joint deterioration and the progression of OA, when drilling into the subchondral bone.”
“In reality most early OA patients are not yet candidates for knee replacements and, therefore, are being treated arthroscopically for mechanical symptomatic relief—and their cartilage lesions are being debrided. Debridement, therefore, is the most commonly performed treatment today for cartilage lesions.”
“The uniqueness of this study is that it mimics almost precisely our current surgical practice.”
If the Agili-C study shows clear superiority over microfracture and debridement for the treatment of joint surface knee lesions it will truly be a landmark event.
The Agili-C Study
The Agili-C study is a prospective, multicenter, open-label, randomized, and controlled, with adaptive sample size. Its primary endpoint is to show superiority of the Agili-C implant over the current Surgical Standard of Care: microfracture and debridement in the treatment of wide range of joint surface lesions.
The investigators plan to enroll a minimum of 250 patients at sites in the United States, Europe and Israel.
Enrollees will be evaluated at 2 weeks after treatment, then again at 3, 6, 12, 18 and 24 months.
Investigators will be using KOOS, IKDC Knee Examination Form 2000, IKDC Subjective Knee Evaluation, SF-12 Health Survey, Tegner Activity Score, Anterior-Posterior (A/P) and Lateral knee X-rays and MRI’s to conduct their evaluations.
The inclusion criteria are the broadest ever in a knee study. Enrollees can:
- Be between 21-75 years old
- Have up to 3 treatable joint surface lesion(s), ICRS Grade III or above, on the femoral condyles and/or trochlea
- Have a symptomatic total treatable area of as much as 1-7 cm2, in both arthritic and non-arthritic knees.
What Is Agili-C and How Is It Implanted?
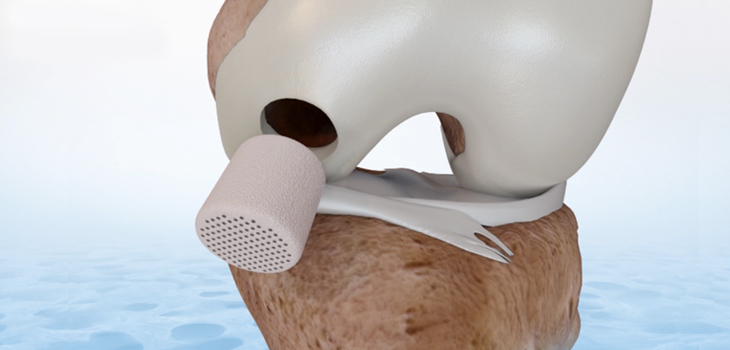
The Agili-C is a biocompatible and biodegradable tapered-shaped solid implant. It is manufactured from aragonite (calcium-carbonate), derived from sea coral. When implanted into a pre-prepared osteochondral hole it acts as a 3D scaffold that potentially supports and promotes the regeneration of the articular cartilage and its underlying subchondral bone.
In previously published animal studies, Agili-C demonstrated the ability to regenerate hyaline cartilage—as confirmed by the presence of Type II collagen and proteoglycans, and the absence of Type I collagen—without relying on growth factors, or external stem cells.
One of the key attributes of Agili-C’s 3D scaffold is its interconnected porosity which maximizes cell contact and promotes matrix deposition.
The implant looks like this:
" data-large-file="https://i0.wp.com/ryortho.com/wp-content/uploads/2019/05/GettingCartilage_CartiHeal_WEB.jpg?fit=730%2C350&ssl=1" src="https://i0.wp.com/ryortho.com/wp-content/uploads/2019/05/GettingCartilage_CartiHeal_WEB.jpg?resize=730%2C350&ssl=1" alt="" width="730" height="350">Courtesy of CartiHeal
“Basically, what CartiHeal designed with the Agili-C is an implant with ideal porosity that enables simultaneous regeneration of the articular cartilage and remodeling of the subchondral bone,” explained Dr. Verdonk. “These micro holes on top of the biomaterial actually created an environment that is very similar to a controlled microfracture in very small, porous, well-defined and non-variable micropores.”
“I have used this implant for many years and in many patients as part of previous clinical studies. I personally think that its most important capability lies in its potential to restore the subchondral bone, which often is the main source of pain, especially in early osteoarthritis,” added Dr. Kon.
Implanting Agili-C, says Dr. Verdonk, is surprisingly simple. “The procedure to implant Agili-C is very close to what the orthopedic surgeon is used to, i.e., drill the hole, place the implant and push it in. Very user-friendly procedure. Only few minutes per implantation.”
“We also found that it’s very important that the entire implant is surrounded by bone—that it touches bone everywhere. When that happens, it gives incredible etiology and normal reconstruction of the subchondral bone and beautiful hyaline cartilage.”
Dr. Zaslav agrees, “Putting in the Agili-C is very easy. It’s an off-the shelf implant with five years shelf life. It’s an outpatient procedure. One of the nice things is the company developed its own tools to make this a perfect press fit and because it’s a rigid implant, it has to be sunk a little bit below the cartilage, so it doesn’t scratch the other surface. But cartilage will grow in to fill that defect.”
“It’s really an easy, 5-step process to put these plugs exactly in a perfect fit.”
Data Due Dates
Agili-C is a CE marked implant. Prior to this FDA IDE (investigational device exemption) study, it had been implanted in several hundred patients in a series of clinical studies in Europe. These studies were all prospective, multicenter, open-label, and controlled.
The first Interim Analysis of the current study is expected at the beginning of 2020.
If Agili-C proves to be statistically superior over microfracture and debridement techniques for repairing cartilage, especially in the early stages of OA…then, perhaps, it may, finally, achieve the promise of making cartilage repair a routine part of every orthopedist’s practice.
[1]https://clinicaltrials.gov/ct2/show/record/NCT03299959?term=cartilage&cond=knee+arthritis&cntry=US&draw=2&rank=48&view=record
[3] ibid
[4] Crawford DC, DeBerardino TM, Williams RJ 3rd. NeoCart, an autologous cartilage tissue implant, compared with microfracture for treatment of distal femoral cartilage lesions: an FDA phase-II prospective, randomized clinical trial after two years. J Bone Joint Surg Am. 2012 Jun 6;94(11):979-89. doi: 10.2106/JBJS.K.00533.
[5] ibid
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.