Using Mesenchymal stem cells (MSC) derived from bone-marrow, University of Alabama researchers report a 90% inhibition of bone carcinoma tumor growth.
Stem Cells Inhibit Bone Carcinomas
5 min read Premium comments
The study, which appeared in the December 1, 2009, issue of Clinical Cancer Research, had nine authors but the lead researcher was Dr. Diptiman Chanda from the Department of Pathology at the University of Alabama.
His hypothesis was that the ability of MSCs to differentiate into osteoblasts (the single nucleus cells that grow bone) could, in a very clever way, obstruct bone cancer cells.
You say Osteoblasts, I say Osteoclasts…let’s work the whole thing out.
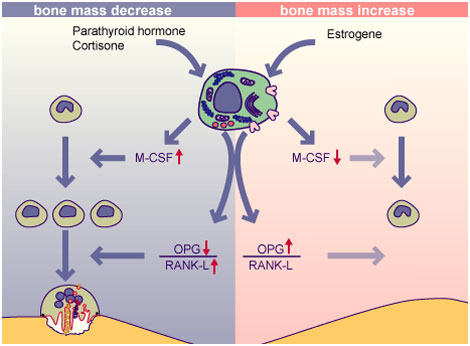
First, it’s important to know what osteoblasts are and what they do. Osteoblasts produce the raw material for bone including a particular family of proteins—bone sialoprotein and osteoprotegerin (OPG). Dr. Chanda focused on that last item—the osteoprotegerins (OPG). Osteoprotegerins are a type of protein or cytokine that blocks the interaction between bone creating cells (osteoblasts) and bone absorbing cells (osteoclasts). Bottom line, OPG can slow down or even stop bone loss.

Osteoblasts creating rudimentary bone
tissue | Source: self-made
Author: Robert M. Hunt |PermissionWhat does this have to do with bone cancer? It turns out that OPGs are a “decoy” receptor for one of the key chemical links (RANKL) responsible for bone maturation and resorption. Dr. Chanda’s hypothesis was that MSCs, which express OPG, could interrupt this bone maturation link and, as a result, also interrupt bone metastasis or cancers.
Bone cancers are often successors to such cancers as breast cancer or prostate cancer. Dr. Chanda’s research is in prostate cancer and that, of course, has led him and his colleagues to digging into the mechanisms of osteoblasts and osteoclasts.
So, when a pancreatic or breast cancer metastasizes into a bone cancer, one of the markers that physician’s look for is osteolysis—or the rate at which bone is resorbed into the body. If bone is disappearing at an overly rapid rate or is being resorbed at an unusual rate, that’s a sign of disease.
The most current clinical research into bone cancer is showing that prostate cancer generated osteoblast lesions are preceded by osteolysis. Therefore, Dr. Chanda hypothesized: preventing osteolysis with the OPG protein from Mesenchymal stem cells would reduce complications of bone metastasis.
That’s the idea at any rate.
Testing, testing, hypothesis testing!
Now for the test. Drs. Chanda, Isayeva, Kumar, Hensel, Sawant, Ramaswamy, Siegal, Beatty and Ponnazhagan went to work. Obviously, it takes a village to do MSC research.
Here is the hypothesis: Unmodified mesenchymal stem cells can prevent osteolytic bone lesions and therefore interrupt the bone carcinoma process.
Here’s the study design: Human prostate cancer cells (line PC3) were implanted into the tiny little tibia bones of severely immunodeficient mice. These are mice that are genetically engineered to be unable to mount, coordinate or sustain an immune response to disease. These are mice, in other words, that are really helpful for disease research. They get sick fast. And they get sick precisely in the way that researcher need in order to test drugs and other biotech therapies for dozens of disease states—including cancers and the autoimmune diseases.
In this test, very quickly after receiving the human prostate cancer cells, the immunodeficient mice developed raging bone carcinomas in their tibias. One day after injecting the mice with human prostate cancer cells (PC3) Dr. Chanda and his colleagues then injected unmodified human Mesenchymal stem cells (derived from bone marrow) into the mice. Unmodified means that the MSC’s were not cultured or changed. They were the same as bone marrow stem cells that surgeons routinely use and rely on when they aspirate bone marrow from their patients in surgery.
The MSCs were injected and immediately went to work expressing OPG—the study protein. The researchers tracked the progression of the OPG proteins using some very sophisticated markers—bioluminescence imaging, micro–computed tomography, immunohistochemistry, and histomorphometry.

Three osteoblast visble at 400x in developing bone
Source: self-made
Author: WbensmithHere’s the fascinating part; not only were the tibia tumors inhibited by the OPG expressed by the Mesenchymal stem cells, but each mouse had new woven bone forming around the tumor cells in the tibia. That new woven bone prevented osteoclasts genesis! And the results were highly statistically significant (P < 0.001).
Using the bioluminescence and other tracking technologies the researchers noticed that the MSC’s “homed” into the metastatic sites as if they were specifically drawn to the cancerous inflammation. Once at the location, the MSC’s then began to “read” the surrounding signals and started to change and differentiate into osteoblasts. As the MSC’s were changing from undifferentiated stem cells into bone osteoblasts, they released osteoprotegerin (OPG). The OPG, in turn, successfully acted as the “decoy” receptor to RANKL, the ligand link for bone maturation and osteoclast proliferation, and disrupted the tumor activity.
Result: 90% Tumor Inhibition!
At four weeks post-injection, there was 90% inhibition of bone carcinoma tumor growth using the adult human bone marrow derived Mesenchymal stem cells.
Why does this happen? Dr. Chanda and his colleagues are hypothesizing that an absence or lack of the amount of naturally occurring Mesenchymal stem cells in patients set the stage for bone carcinomas. By adding concentrations of MSCs, clinicians have a new weapon in the battle with bone cancers.
After the mice were sacrificed and the bones were studied under microscope, Dr. Chanda and his colleagues noted that the injected adult bone marrow derived Mesenchymal stem cells also acted to preserve trabecular and cortical bone structures in the mice. In addition, the histologies confirmed that osteoclast proliferation had been inhibited.
Finally, the researchers ran one more test to really check to see if the MSCs were truly as effective as they seemed to be. This was, in effect, a dose response test. Where the researchers injected MSCs into the mice tumors one day after the tumors were triggered, in this follow up test, the researchers waited two weeks before injecting MSCs.
Indeed, when adult human MSCs were injected two weeks after the PC3 cells were injected, the mice outcomes deteriorated as compared to the first test. Specifically, when injected two weeks after PC3 cells were introduced, the MSCs were NOT effective in inhibiting tumor growth. Testing further at one week post PC3, the injections of MSC’s successfully resulted in new, woven bone which then surrounded the tumor. Chanda and his colleagues then subjected the new woven bone to mechanical strength testing and found that it was similar in strength to normal bone.
Another critical conclusion reached by the researchers is that the ability of the injected adult MSCs to differentiate into bone cells (osteoblasts) was NOT due to the increased expression or upregulation of bone growing genes (osteogenic genes). Instead, said Chanda, it was likely due to the abnormally high rate of bone maturation and loss—enhanced osteoclastogenesis in other words—and that the MSCs somehow sensed that and began to change and express OPG accordingly.
Dr. Chanda primary conclusion, of course, is that MSCs can play a very effective role in reducing the tumors from bone carcinomas. The researchers’ secondary conclusions were that the clinical task when confronted with a patient with a bone carcinoma is to find ways to augment the patient’s existing store of MSCs. If a shortage of MSCs creates the conditions for bone carcinomas in patients with breast or prostate cancers, then injections of either autologous (bone marrow or adipose derived) stem cells or allograft stem cells could well slow or arrest the progression of bone carcinomas.
For more information – Clin Cancer Res 2009;15(23):7175–85 Chanda D, Isayeva T, Kumar S, Hensel JA, Sawant A, Ramaswamy G, Siegal GP, Beatty MS, Ponnazhagan S.
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.