For millions of chronic low back pain sufferers, the road to relief has long resembled a blindfolded stumble through a diagnostic minefield. But now, a team of spine specialists has introduced a breakthrough roadmap—a structured algorithm that may finally shine a light on one of back pain’s most elusive culprits: lumbar discogenic pain.
Published July 1, 2025, in the Journal of Pain Research, the paper, titled "A Proposed Diagnostic and Treatment Algorithm for the Management of Lumbar Discogenic Pain"—by Morgan P. Lorio, D.O. (Orlando College of Osteopathic Medicine), Jon E. Block, Ph.D. (San Francisco private practice)—delivered a methodical yet practical way for clinicians to identify, categorize, and treat what could account for up to 70% of all chronic low back pain cases.
The lead architects behind this initiative? Spine and pain medicine veterans Morgan P. Lorio, D.O., of the Orlando College of Osteopathic Medicine, and Jon E. Block, Ph.D., a San Francisco-based clinical researcher.
Backed by a dozen top-tier coauthors (Douglas P. Beall, M.D.; Thomas J. Myers, M.D.; Ramana K. Naidu, M.D.; W. Porter McRoberts, M.D.; Timothy T. Davis, M.D.; Emmanuel G. Gage, M.D.; Aaron K. Calodney, M.D.; Paul Verrills, M.D.; Michael J. De Palma, M.D.; and Kasra Amirdelfan, M.D), they harnessed a modified Delphi consensus process—a structured method of expert agreement—to construct the algorithm.
And the timing couldn’t be better. In 2023, discogenic pain finally got its official stamp of legitimacy when ICD-10-CM codes were created specifically for it. That bureaucratic milestone signaled what clinicians have long suspected: discogenic pain isn’t just real—it’s rampant.
Discogenic Pain, Demystified
If you’re imagining discogenic pain as that vague ache that flares up when you sit too long, you’re not wrong. The pain is typically axial and midline, worsens with lumbar flexion and sustained hip bending, and is notoriously difficult to localize. Unlike sciatica, it doesn’t shoot down the legs—so it often gets misclassified as muscle strain or general “low back pain.”
And misclassification? That’s where things go off the rails—leading patients down rabbit holes of inappropriate therapies or unnecessary surgeries.
Enter the algorithm.
A Step-by-Step Spine Strategy
The algorithm kicks off with a thorough physical exam. If the patient reports:
- Pain rated ≥ 4/10
- Discomfort with lumbar flexion
- Inability to sit comfortably for 30 minutes or more
- Pain provoked by sustained hip flexion
- Yet normal neurological findings
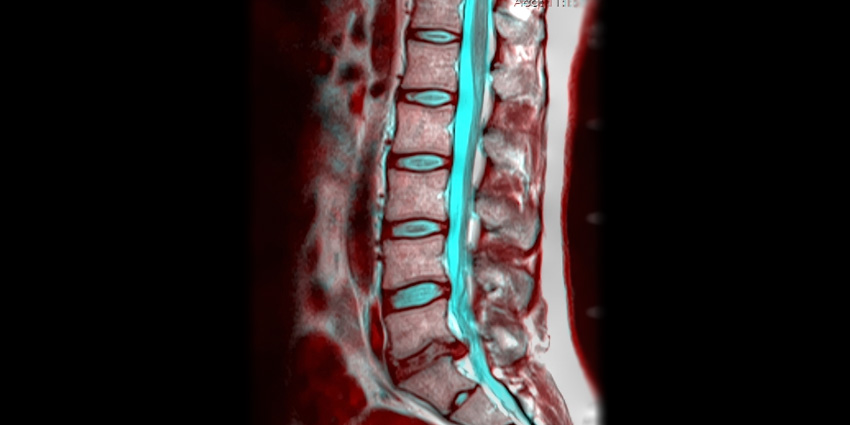
…and the symptoms have lasted six months or longer, it’s time to bring in the big guns: imaging.
A T2-weighted sagittal MRI is the go-to tool here, evaluated using a modified Pfirrmann scale, which grades disc degeneration from 1 to 8:
- Grades 1–2: No need to panic—conservative therapy like physical rehab and behavior modification may do the trick.
- Grades 3–7: Time to consider intradiscal interventions—think platelet-rich plasma (PRP), mesenchymal stromal cells, or nucleus pulposus allografts.
- Grade 8 or no relief from earlier steps? Surgical options like spinal fusion or disc arthroplasty enter the chat.
And if Modic type 1 or 2 changes show up on MRI? The authors give a nod to basivertebral nerve ablation—a minimally invasive option gaining traction when nothing else seems to help.
Treatment success is pragmatically defined: a 30% or greater pain reduction within 6 months (or 12 months if surgery is involved).
A Collaborative, Disc-Saving Approach
One of the most promising aspects of this model is its collaborative ethos. The authors don’t champion any one specialty over another. Instead, they propose a multidisciplinary team—spine surgeons, radiologists, and interventional pain docs—working together to tailor treatments and avoid reflexively jumping to surgical solutions.
This could be a huge win for patients stuck in diagnostic limbo—or for those who want options before going under the knife.
And as disc-preserving technologies (like motion-restoring surgery and cutting-edge biologics) gather steam, clinicians finally have a framework grounded in consensus and real clinical utility.
The Takeaway?
This isn’t just another theoretical flowchart to gather dust in a textbook. It’s an actionable blueprint that could cut through the diagnostic noise, reduce inappropriate treatments, and actually help people get better.
With structured guidance like this, the days of shrugging at vague “low back pain” may finally be numbered.
Stay tuned—and maybe sit up a little straighter while you wait.