Hip instability. Despite an elegant surgical approach, perfect cup positioning, meticulous soft tissues balancing, dislocation remains a frustrating, humbling complication after total hip arthroplasty (THA).
Large Joints and Extremities Premium
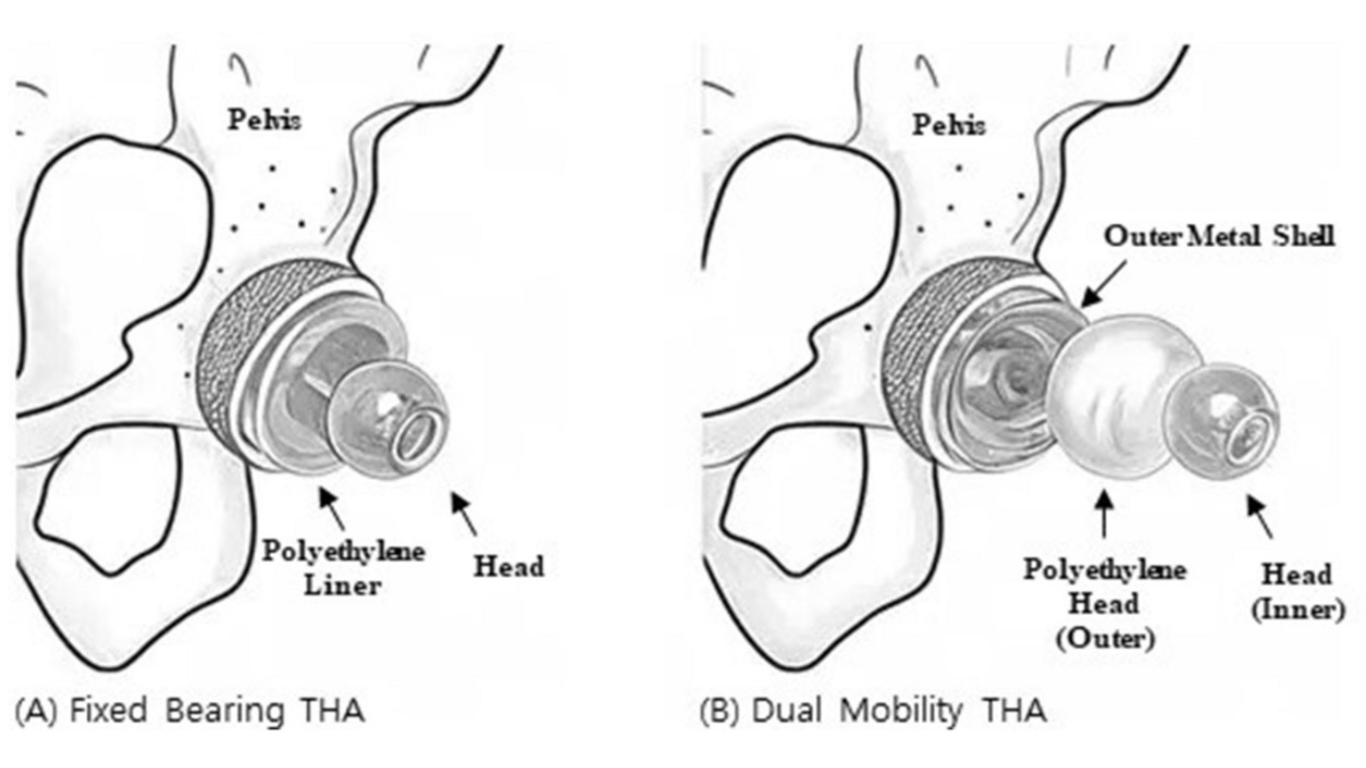
Dual Mobility vs. Jumbo Heads in Primary THA
1 min read Premium comments
StudiesPremiumdual mobility implantship instabilityJournal of Arthroplastyprimary total hip arthroplasty
Author
React: