Does changing the shape of the cannula, to a rectangular shape, for example, deliver a consequential improvement in spine surgery, in a transforaminal lateral interbody fusion, for example?
New Data for More Graft and Nerve Avoidance in TLIF
3 min read Premium comments
Secondary#transforaminallumbarinterbodyfusion#implantplacement#kg2surgesystem#kleinerdevicelabs
The answer, and it is an intriguing one when you dig into the “why,” is “yes.”
The device in question, KG™2-Surg(r) Flow-Thru, invented by spine surgeon Jeff Kleiner, M.D., is the subject of a couple of new studies and anecdotal data which support not only that proposition that a rectangular cannula combined with a biportal conduit for graft delivery will put more graft in the disc space but that it will also improve fusion rates and by extension patient outcomes.
Minnesota-based orthopedic surgeon, Nathan Wanderman, M.D. told OTW, “I have been using KG2 for a year and have yet to encounter a pseudoarthrosis. I have been surprised at how much more graft I can get into disc spaces with the device, and there is an appreciable difference in graft volume compared to products I have used in other settings.”
As Dr. Kleiner explained to OTW, “The KG2 system relies upon a rectangular graft cannula pre-attached to an I-Beam implant that doubles as a biportal conduit for graft delivery. It has no pinch points and allows implant insertion and grafting with a single pass of an instrument. This is distinct from the multi-step process involving round, end-dispensing funnels that poorly distribute graft, are prone to underfill the disc space and give surgeons a feeling of ‘graft insecurity.’ These archaic systems require flowable graft, frequently jam and are prone to diminished endplate-to-endplate contact, which ultimately results in a failure to heal.”
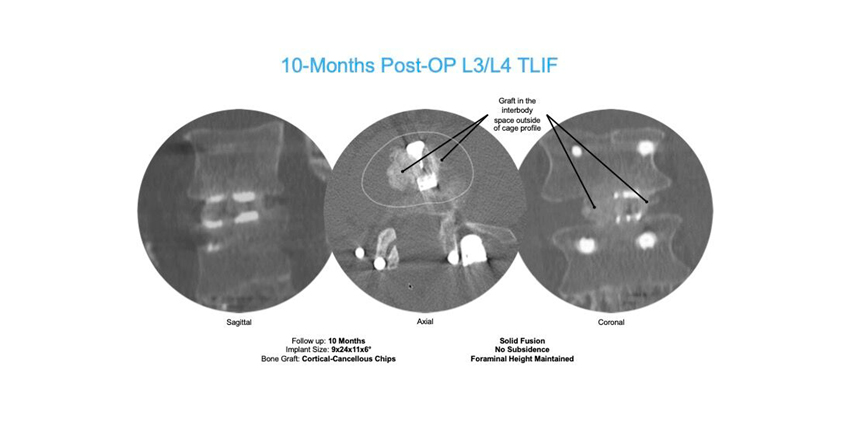
“This example of a patient CT scan 10 months post-surgery (see images above) utilizing the KG2 Surge for a TLIF procedure shows obvious fusion and demonstrates the value of a biologic foundation of graft between vertebral end plates, maintaining disc height, preventing implant subsidence and preservation of foraminal height”, said Dr. Jeff Kleiner, founder and CEO of Kleiner Device Labs. “The importance of that biologic foundation was highlighted in the recent release of a study by the University of Toledo showing the higher failure rate of spinal fusions in diabetic patients.”
75% More Cross-Sectional Area for Graft
Dr. Kleiner says he was frustrated by this flawed technology and knew there was a better way.
“I set out to eliminate some headaches for my colleagues—and for myself,” Dr. Kleiner told OTW.
“I knew it would be important to use a dispensing device that matches the annulotomy—hence, the KG 2 rectangular cannula that has 75% more cross-sectional area for graft, and biportal delivery in a distracted disc space that prevents jamming. With the KG 2 Surge, surgeons can deliver a variety of graft materials, meaning that the graft material doesn’t have to have a primary characteristic of flowability. Surgeons are free to select a graft that has the greatest osteogenic and osteoconductive properties.”
“While BMP may be an alternative, it has a prohibitive cost and is associated with substantial risk. There are many potential deleterious side effects of BMP that can be obviated by maximizing the graft volume that the KG 2 system provides.”
Concerning diabetic patients, Dr. Kleiner told OTW, “We know that diabetes and other endocrinopathies impact the patient’s ability to heal a fusion. The KG2 Surge offers optimal placement and quantity of bone graft with a single instrument pass. This is especially important for individuals with diabetes, who are prone to fusion failure and infection.”
2.5x More Graft, No Touching, Nerve Avoidance
Dr. Kleiner: “With our system, if you ‘do good carpentry,’ i.e., clear out the disc material to make more room for the graft, then you can put in 2.5x more bone graft than with conventional means. In addition, because this is a ‘touch free’ technology and since the implant and disc are not pre-packed, the risk of implant cross-contamination is essentially eliminated. With the pre-assembled, single patient use KG2 Surge, redundant operative steps are reduced, diminishing the risk from multiple passes by the nerve tissue and reducing the risk of soft tissue irritation/damage.
Dr. Kleiner told OTW, “In 2016 I published on my minimally invasive spine surgeries done with a typical round dispensing device, finding that my fusion rate was 75%. I have found that by using our rectangular cannula I can put in more graft material and my fusion rate increased by 17%! To date, the KG2 Surge has been used in 130 patients—and although it is early in the process, no fusion failures have been reported.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.