According to a just published, double blinded, randomized clinical study of three of the most popular patella resurfacing implants (onlay, inlay and onlay oval) … one design appears to deliver better patient outcomes than the other two! And one design is clearly inferior!
To Resurface the Patellar: Onlay, Inlay or Onlay Oval?
3 min read Premium comments
Secondary#axialalignment#implantsizing#patellarresurfacing
The outcome of this study from a Sydney, Australia based research team at Sydney Knee Specialists, “Does Choice of Patellar Implant in Total Knee Arthroplasty Matter? A Randomized Comparative Trial of 3 Commonly Used Designs,” appears in the December 9, 2022, edition of The Journal of Bone and Joint Surgery.
“If you decide to resurface, surgeons need some clarity on what implant design they should use,” explained co-author Samuel MacDessi, M.B.B.S., Ph.D., with Sydney Knee Specialists, to OTW.
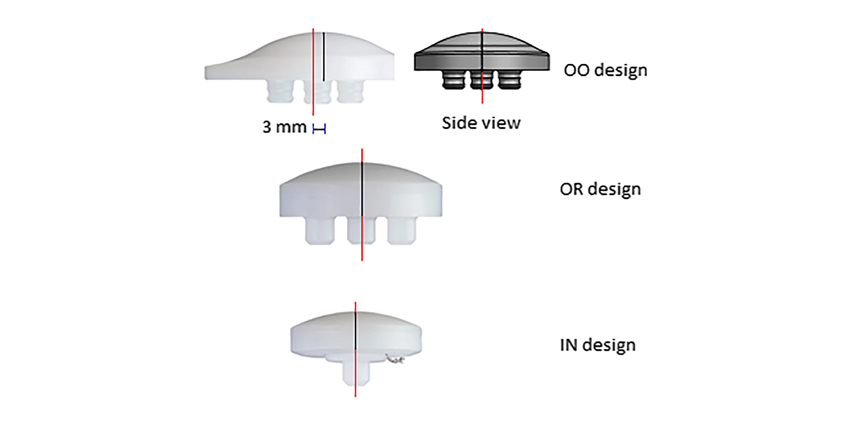
“There are three implants used to resurface the patella, and all of these, inlay, onlay round and onlay oval are commonly utilized. But to date, it was unknown if one type of implant design was superior to the others. So, we designed a randomized controlled double blinded trial to understand what implant design may be best for patients undergoing primary TKA using the same posterior-stabilized prosthesis.”
The researchers followed patients who had TKA for primary osteoarthritis for a minimum of two years, with survivorship outcomes followed for a mean of five years. The primary outcome was the Kujala score, a 13-question tool used to quantify patellofemoral disorders (range of 0 to 100 points).”
“The secondary outcome was the Knee injury and Osteoarthritis Outcome Score—five domains: knee-specific pain, other symptoms, function in activities of daily living, sport and recreation, and knee-related quality of life.
The team enrolled 122 patients into the study and randomized them to one of the three designs.
Kujala score rates were 97.5% for the inlay group, 100.0% for the onlay round group, and 97.5% for the onlay oval group.
“Despite this study showing no differences in the primary endpoint of change in Kujala score, there were multiple secondary outcomes that were improved with use of onlay implants,” Dr. MacDessi told OTW.
“Specifically, at up to two years, we found improved patient report outcome scores in some of the Knee injury and Osteoarthritis Outcome Score subscales with use of onlay round implants.”
“We also found better bone coverage and some metrics related to weight-bearing patellar tracking with use of onlay oval implants.”
“Inlay implants that retain a rim of the osteochondral surface failed to confer any benefit over the other designs in any clinical, scinitigraphic, or radiographic outcome at two years, and no benefit in survivorship or adverse event rates at five years.”
“When these patient-centered outcomes are collectively considered, in conjunction with a long-term survivorship advantage with onlay designs from separate national registry data, these results suggest that an onlay design may be preferable if the patella is to be resurfaced.”
“It has long been understood that patellofemoral outcomes are not purely related to patellar resurfacing alone. Femoral prosthetic morphometry, implant sizing, axial alignment, and alterations to patellofemoral offset have all been associated with outcome differences from this very complex joint. The debate on whether to resurface the patella will continue.”
“Admittedly,” said Dr. MacDessi to OTW, “we were not anticipating any differences between the three designs. The finding that retention of native rim of cartilage and bone with the use of the inlay implant was the worst of all three did surprise us.”
“Many surgeons use this type of implant because it is considered a relatively easy ream-in method versus resection technique. It also does not run the risk of over-resection. However, it may be that leaving only half of the retropatellar surface covered with this type of design may be the issue here.”
“The major criticism of this study was that we did not include a non-resurfaced arm and future research should definitely address this. Larger studies, potentially nested in national registries, and including different prostheses will also be of value.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.