What are the complications and risk factors associated with treating fixed sagittal imbalance with spinal osteotomy? A new study from Hospices Civils de Lyon in Lyon, France, has answers.
What Are Common 3-Column Spinal Osteotomy Risk Factors?
2 min read Premium comments
Secondary#sagittalimbalance#sagittalverticalaxis#spinalosteotomy
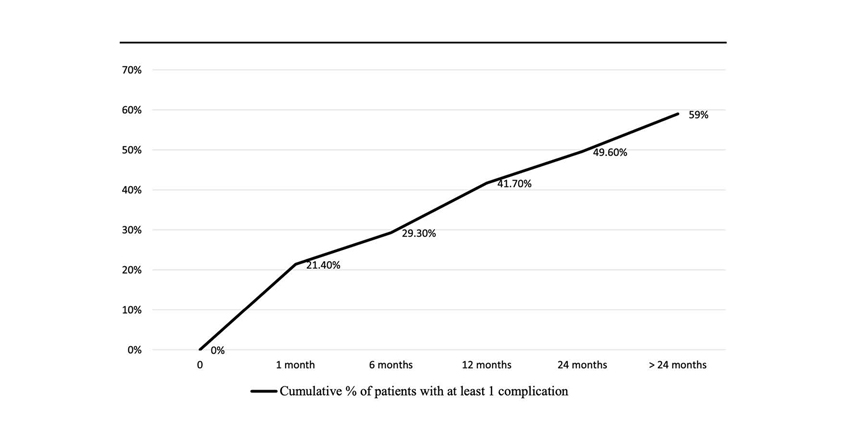
" data-large-file="https://i0.wp.com/ryortho.com/wp-content/uploads/2022/10/WhatAreCommon_ComplicationFree_WEB.jpg?fit=850%2C478&ssl=1" src="https://i0.wp.com/ryortho.com/wp-content/uploads/2022/10/WhatAreCommon_ComplicationFree_WEB.jpg?resize=850%2C478&ssl=1" alt="" width="850" height="478">Complication-Free Survival / Source: European Spine Journal and Cédric Barrey, M.D., Ph.D.
The new study, “Factors influencing complications after 3-columns spinal osteotomies for fixed sagittal imbalance from multiple etiologies: a multicentric cohort study about 286 cases in 273 patients,” was published in the October 3, 2022 edition of the European Spine Journal.
The researcher team designed a blinded retrospective analysis of prospectively collected data from patients who had been treated with a 3-column spinal osteotomy (this was a multi-center study, 7 hospitals, all blinded, participated) between January 2010 and January 2017. The team then collected both clinical and radiological data pre- and postoperatively.
Two hundred seventy three patients were enrolled, representing 286 osteotomy procedures. The team collected 1-year follow-up data, both clinical (Visual Analogue Scale pain, Oswestry Disability Index and Scoliosis Research Society-22 scores) and radiological (sagittal vertical axis, spino-sacral angle, loss of lordosis and pelvic version) parameters.
Co-author Cédric Barrey, M.D., Ph.D., a neurosurgeon with the Hospices Civils de Lyon, told OTW, “A total of 164 patients (59.2%) experienced ≥ 1 complication during the follow-up period, with a total of 277 complications. Survival rates without complications were 57.4%, 47.4% and 30%, respectively, at 1, 2 and 5 years.”
“Most complications were mechanical (35.2%), typically occurred more during the follow-up period than immediately after the surgery, and primarily consisted of pseudarthrosis and rod breakage. Other complications were general (17.6%), surgical site infection (17.2%) and neurological (10.9%).”
Regarding neurological issues, the authors wrote, “Prevention of those complications might be done while enlarging the canal centrally, reducing fibrosis in revision surgery, searching for posterior bony contact in osteotomy closure and using a temporary rod in VCR to control any translation.”
“Preoperative neurological status, operative time (+ 19% of risk each additional hour) and combined surgery were assessed as risk factors for overall complications.”
As for something protective against complications, Dr. Barrey stated to OTW, “The use of patient-specific rods appeared to be significantly associated with less overall complications.”
The authors note that their study is important not only because in involved seven different clinical sites, but because it involves a large number of patients (273), whereas most studies in this arena have been based on data with less than 100 patients.
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.