New work from Stanford University asked, “What is the maximum force that can be applied during retraction of the piriformis tendon to expose the hip during total hip arthroplasty?”
How Much Force Will Damage Piriformis Muscle? Shockingly Little.
2 min read Premium comments
#totalhiparthroplastySecondary#piriformissparingapproach#piriformistendon
The answer: “not much.”
The study, “A Small Amount of Retraction Force Results in Inadvertent Piriformis Muscle Damage During a Piriformis-Sparing Approach to the Hip,” appears in the October 7, 2020 edition of The Journal of Bone and Joint Surgery.
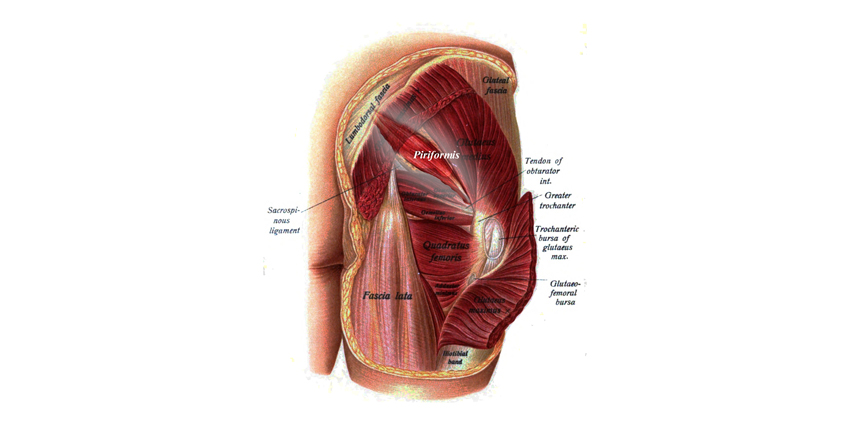
“During a piriformis-sparing THA [total hip arthroplasty], the piriformis tendon must be retracted to provide line-of-sight access to the femur and acetabulum. To our knowledge, the upper limit of the force, rate of loading, and duration of loading that may damage the piriformis musculotendinous complex during retraction has not been quantified,” wrote the authors.
In this study, the authors used a patent-pending instrumented retractor to record the applied force, duration, and angle of retraction during a piriformis-sparing approach. There were 23 hips dissected from 16 cadavers
Co-author Derek Amanatullah, M.D. is with the Department of Orthopaedic Surgery at Stanford Medicine in Redwood City, California. He told OTW, “I never understood how providers were concerned about how the tension of a piriformis tendon repair after release might affect the sciatic nerve and others would just retract the piriformis tendon without consideration. This suggested to me that the trends of minimally invasive surgery had been taken too far.”
In 22 of the hips (96%) there was no damage to the piriformis tendon during retraction for visualization of the hip. There was, however, complete or partial damage to the piriformis muscle at the sacral origin, belly, or musculotendinous junction in 21 of the 23 hips.
The authors stated, “The mean peak force to failure of the piriformis muscle was exceedingly small (29.0 ± 9.4 N; range, 10.1 to 44.9 N). The mean peak force applied to the piriformis retractor is much less than the force required for several common daily activities, such as opening a door or crushing an empty aluminum can…”
Dr. Amanatullah commented to OTW, “Inadvertent soft tissue damage is not routinely accounted for when accessing the invasiveness of a procedure, so it is no longer adequate to define minimally invasive surgical procedures simply as an approach that involves the limited release of anatomical structures. The use of instrumented retractors re-defines surgical invasiveness by providing data that could alter our understanding of the soft tissue damage caused by retraction and open the possibility of robot-assisted or damage-limiting retractor systems.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.