Can a novel, versatile mathematical model of the knee joint shed light on the effects of total knee arthroplasty (TKA) design and surgical conditions on TKA outcomes? A team from the University of Tennessee put a promising 12-point mathematical modeling to the test. Here is what they learned.
Validated 12-Point Knee Mathematical Model Announced
2 min read Premium comments
#totalkneearthroplastySecondary#tka#bonedeformity
Their study, “A Validated Forward Solution Dynamics Mathematical Model of the Knee Joint: Can It Be an Effective Alternative for Implant Evaluation?” was published in the November 1, 2020 edition of The Journal of Arthroplasty.
Richard D. Komistek, Ph.D., the Fred M. Roddy Professor of Biomedical Engineering and
co-center director of the Center for Musculoskeletal Research at the University of Tennessee, and study co-author explained the genesis of the study to OTW, “Although TKA is a very successful procedure, there remains a subset of patients that demand more from their implant and are not completely satisfied.”
“This model can evaluate any TKA design within many TKA subjects, including bone deformity, varying alignment, surgical technique and component placement. The results from these simulations allow us to assess variability and factors that may contribute to clinical success or concern.”
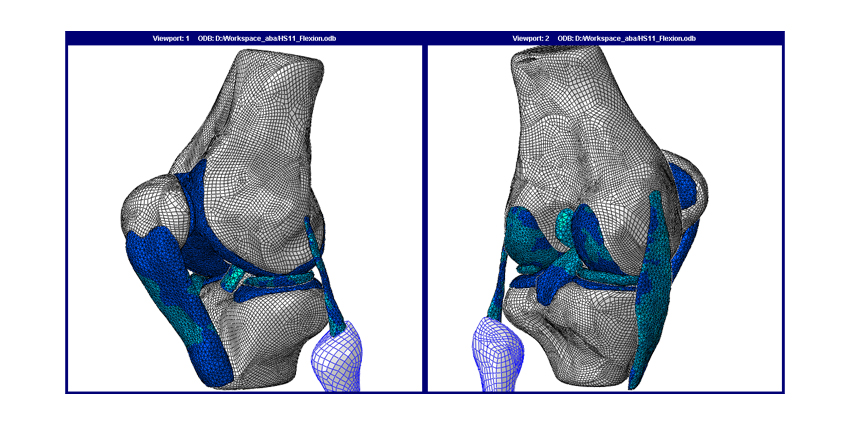
In developing their 12-point model, the researchers brought patient-specific three dimenstional bone models and TKA implant computer-aided designs into the model. “The mass of each body segment is input as a percentage of the whole-body mass based on the literature. The modeled knee joint has 12-DOF [degrees of freedom]: a 6-DOF femorotibial joint and a 6-DOF patellofemoral joint. The muscle controller and contact detection algorithm compute forces to drive the translational and rotational motion of the knee joint.”
Dr. Komistek and his colleagues also incorporated three major active knee muscles into the model: quadriceps, hamstring, and gastrocnemius (other soft tissues were treated as stabilizers). They also included the anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, lateral collateral ligament, patellar ligament, lateral patellofemoral ligament, medial patellofemoral ligament, and medial patellomeniscal ligament.
Because this new mathematical model incorporates a graphical user interface, users can alter TKA parameters and do sensitivity analyses to determine the effects of specific parameters on surgical outcomes.
“Results from the model correlated well with fluoroscopic studies where TKA assessments lead to decreased axial rotation, condylar rollback and weight-bearing flexion compared to the normal knee,” said Dr. Komistek to OTW. “Modification to component placement, posterior tibial slope, design changes and implant conformity can lead to improved knee mechanics.”
“Our research team believed that new tools should be developed to evaluate new knee implant designs before they are implanted in the body, allowing for a quantifiable assessment. Therefore, having a validated mathematical model that can predict clinical outcomes could be a valuable asset in evaluating new knee implant designs.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.