Would you stop a routine practice if it did not affect quality and resulted in a substantial savings? But of course!
Drop Metabolic Panels After TJA?
2 min read Premium comments
Secondary#metabolicpanel#outpatientarthroplasty
New work from Johns Hopkins suggests a new way to do just that. The study, “Routine Basic Metabolic Panels Are Not Needed in All Patients After Primary Total Joint Arthroplasty: An Opportunity for Cost Reduction,” was published in the August 10, 2020 edition of The Journal of Arthroplasty.
Robert S. Sterling, M.D., associate professor at Johns Hopkins University in Baltimore, Maryland, and co-author on the study, explained the impetus for this work to OTW. “Our program routinely reviews our clinical practices to ensure that we are keeping up to date with current best evidence. As we started to transition to some same day discharges at our hospital and with the rise in outpatient arthroplasty across the country, we recognized that routine post-op labs obtained in the hospital on all patients are not part of the outpatient protocol. There are other surgical areas that have explored routine labs and we saw this as an opportunity to provide some evidence to help guide us to a safe practice.”
The authors reviewed 802 cases (758 patients) of primary lower-extremity total joint arthroplasty (TJA) performed from January 1 through December 31, 2018 at the Johns Hopkins tertiary care medical center. The researchers calculated the Age-Adjusted Charlson Comorbidity Index values, as well as the institutional costs of one basic metabolic panel (BMP) and of all basic metabolic panels not prompting intervention.
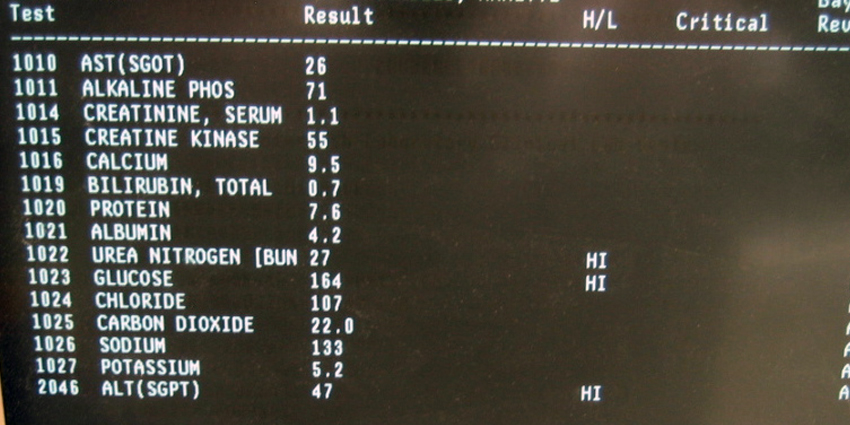
The team found that their institutional cost for a basic metabolic panel was $36. Of the 1,032 postoperative basic metabolic panels ordered, 958 (93%) prompted no intervention. The authors wrote, “This equated to $34,488 of avoidable BMP costs. We identified 27 cases (3.4%) requiring intervention secondary to abnormal BMPs. Independent predictors of intervention were preoperative renal dysfunction (i.e., abnormal creatinine or glomerular filtration rate <60 mL/min), number of current nephrotoxic medications, and AA-CCI [Age-Adjusted Charlson Comorbidity Index] value.”
Because We’ve Always Done It Like That
We asked Dr. Sterling why this issue hadn’t been more thoroughly explored before and he explained to OTW, “I think that this is both an issue of comfort and routine. We have gone through decades of practice where this was the way it was done. As we have continued to question the rote pieces of practice and develop evidence-based guidelines, everything that we do will continue to come into question. This is simply another facet of practice that was very ingrained in our behavior that it was not much questioned in the past.”
Kidney Alert
“The most important takeaway is that we need studies with a larger number of patients to best define which patients should have post-operative laboratory studies. While criteria for outpatient arthroplasty have been written on extensively, surgeons may need to pay close attention to the number of nephrotoxic medications a patient is on when the patient is being considered for outpatient surgery as we found a significant increase of odds of having an abnormal post-op lab value that required an intervention in this patient group in addition to patients with pre-operative renal dysfunction and an increased age-adjusted Charlson Comorbidity Index.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.