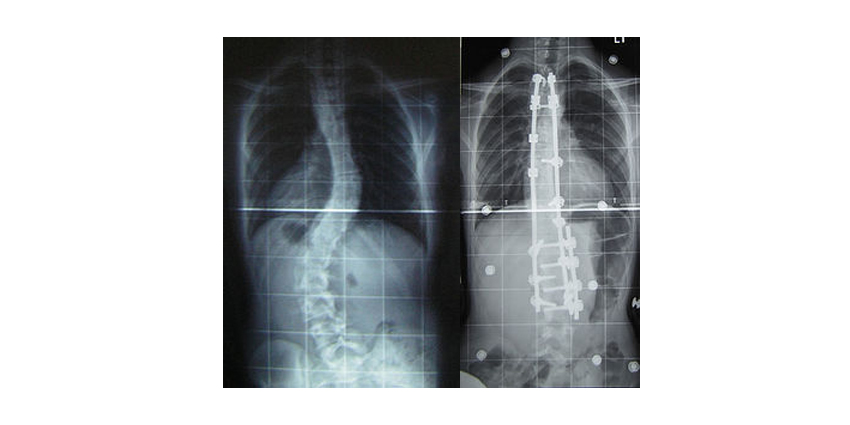
Anyone who has played limbo, or performed corrective surgery for scoliosis has been asked the same question, “How low can you go?” For scoliosis correction, the question refers to the lowest instrumented vertebra (LIV), and how to balance a stabilized fusion with preservation of as many motion segments as possible.
Studies on Selecting the Lowest Instrumented Vertebra for AIS
3 min read Premium comments
Secondary#scoliosis#AIS#touchedvertebra
A recent publication written by a group of surgeons from New York-Presbyterian and Columbia University Medical Center in New York, New York, in conjunction with the Harms Study Group investigated the effectiveness of using the “touched vertebra,” (TV) which is the most cephalad vertebrae that intersects with the center sacral vertical line (CSVL), a vertical line drawn on radiographs straight through the center of the sacrum and up.
The article, “Selecting the “Touched Vertebra” as the Lowest Instrumented Vertebra in Patients with Lenke Type-1 and 2 Curves,” was published in The Journal of Bone and Joint Surgery in August 2020. The work was previously presented at the 2017 Global Spine Congress.
The group retrospectively evaluated radiographs from nearly 300 patients who had at least 5 years of follow-up after correction of Lenke type-1 and 2 adolescent idiopathic scoliosis (AIS) curves. The radiologists identified the touched vertebra, and the lowest instrumented vertebra in each patient’s radiographs. The group then analyzed the CSVL-lowest instrumented vertebra distance, the distance between the CSVL line and a vertical line drawn through the mid-point of the lowest instrumented vertebra, with the lowest instrumented vertebra’s relationship to the touched vertebra (same, cephalad, or caudad). The closer these two lines, the greater the correction achieved.
The authors found that just over half (51%) of the included patients’ lowest instrumented vertebra was their TV, 32% had a lowest instrumented vertebra caudad to the TV, and 17% had a lowest instrumented vertebra cephalad to the touched vertebra. The CSVL-lowest instrumented vertebra distance was significantly greater for patients with a lowest instrumented vertebra cephalad to the TV if the curve type had an “A” lumbar modifier (meaning the CSVL passes between the pedicles of the apical vertebrae). Those with a “B” or “C” modifier did not have a statistically significant difference in the CSLV-lowest instrumented vertebra distance, whether the lowest instrumented vertebra was above or below the touched vertebra.
The group concluded that using the touched vertebra as the lowest instrumented vertebra is an acceptable choice for patients with Lenke type-1 or 2 curves, but those with Type-1A curves should have an lowest instrumented vertebra at least as low as the touched vertebra.
A similar study was published in 2016 by a group from the Department of Spine Surgery at Nanjing University Medical School in Nanjing, China. The article, “Selecting the Last “Substantially” Touching Vertebra as Lowest Instrumented Vertebra in Lenke Type 1A Curve,” was published in Spine (Phila PA 1976).
The authors compared the selection of substantially touched vertebra (STV) versus non-substantially touched vertebra (nSTV) as the LIV for patients with Lenke type-1A curves. They define the STV as the most cephalad touched vertebra when the CSLV passes between, or touches the pedicles. When the CLSV passes outside of the pedicle border, the touched vertebra is defined as nSTV. The group compared 2-year follow-up data for patients whose lowest instrumented vertebra was at the nSTV, nSTV +1, or STV. Distal adding-on, curve progression involving more distal vertebrae, was significantly associated with using the nSTV as the lowest instrumented vertebra, compared with the nSTV+1 or STV.
Both studies find agreement that using an lowest instrumented vertebra cephalad to the touched vertebra is associated with poorer prognosis than using the touched vertebra. However, the Chinese study suggests that if the touched vertebrae is only grazed by the CSLV, the next caudad vertebrae should be considered for the lowest instrumented vertebra to prevent possible curve progression.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.