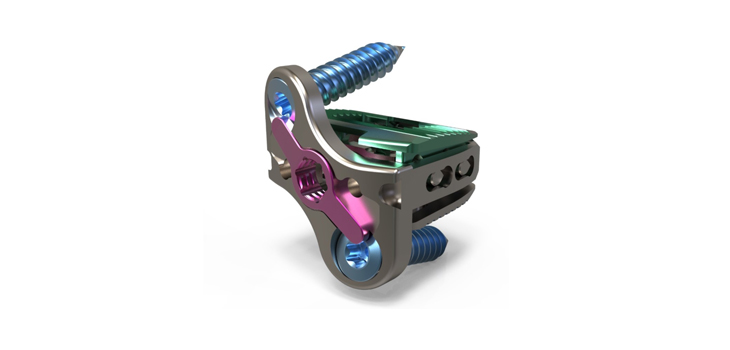
Jupiter, Florida-based Atlas Spine, Inc. has launched its latest interbody device for anterior cervical discectomy and fusion (ACDF) procedures. The HiJAK SA Expandable Cervical Stand-Alone Interbody system builds on the design of the HiJAK AC by adding an integrated, low-profile plate to the expandable interbody device.
Atlas Spine Launches Stand-Alone Expandable Cervical Spacer
1 min read Premium comments
Secondary#atlasspine#hijak#standaloneexpandablecervicalspacer
The HiJAK SA and HiJAK AC allow for custom adjustments to both height and lordosis restoration. The device consists of textured titanium alloy endplates with additional titanium alloy or PEEK components and is currently the only stand-alone, expandable cervical spacer on the market that allows for height and lordosis correction.
Grant Skidmore, M.D. performed the first surgery to implant the device at the Neurological Specialists, Inc. practice in Norfolk, Virginia. Skidmore calls the device a “game changer” for ACDF surgery. “The ease of insertion, restoration of cervical lordosis and perfect alignment of the plate every time make it the pinnacle of technology for ACDF,” he stated in a press release from the company.
Atlas Spine CEO Matt Baynham spoke confidently about the technology in the HiJAK devices, “We’re approaching two years of very positive clinical results with our HiJAK AC expandable interbody, so the merits of the technology have well been validated at this point. This system really offers unmatched capability in an extremely simple to use device. That coupled with its ability to accommodate minimally invasive approaches and reduce surgical times, make the system ideal for outpatient surgery procedures.”
Patrick Senatus, M.D., Ph.D., medical director of minimal invasive and functional spine surgery at Hartford Healthcare in Hartford, Connecticut, previously tested the device. He said, “I had the opportunity to implant and evaluate this technology in a cadaver lab, and I have to say, it doesn’t get much easier than this.”
The HiJAK SA received FDA 510(k) clearance, which OTW announced back in April. The device is indicated for 1- or 2-level ACDF surgery with no additional fixation needed.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.