When researchers from Belgium noticed something amiss with knee joint line orientation after high tibial osteotomies, they decided to investigate. Their work, “Changes in knee joint line orientation after high tibial osteotomy are the result of adaptation of the lower limb to the new alignment,” appears in the June 1, 2020 edition of The Knee.
What Causes Mis-Aligned Knee Joints After Tibial Osteotomy?
3 min read Premium comments
#hightibialosteotomies#kneejointlineorientation
Could orientation stay the same even after large corrections?
Stijn Bartholomeeusen, M.D., an orthopedic surgeon at AZ Herentals Hospital in Belgium and a co-author on the study explained to OTW how knee joint line orientation became the subject of this study: “At first my interest in knee joint line orientation after high tibial osteotomy was triggered by the trend to perform double level osteotomies for large corrections in order to avoid excessive oblique joint line orientation.”
“In our center we perform about 150 high tibial osteotomy surgeries a year and when I looked into the knee joint line orientation on postoperative long leg X-rays of our center I hit upon confusing results regarding the knee joint line orientation changes after osteotomies.”
“More specifically, I saw that in several cases, even after large corrections, the knee joint line orientation did not change at all. When I discussed these findings with several colleagues in my center and beyond (for example during my fellowship with Dr. Kristian Kley and Prof. P. Lobenhoffer in Germany, both experts in performing osteotomy surgery around the knee), I could not get a satisfactory explanation for these findings.”
Is it natural compensation?
“In the literature I noticed these unexpected results were already described by K M Lee et al. and K-J Oh et al. but could not yet be explained. According to these authors these findings might be explained by some kind of compensation mechanisms in the ankle or subtalar joint. However, I could not understand how these mechanisms would influence the knee joint line orientation and I was trying to understand what happened to the lower limb after performing high tibial osteotomy surgery, again something no one was able to thoroughly explain.”
To find out what might be happening, Bartholomeeusen and his team examined multiple parameters (preoperatively and three months postoperatively) for 117 high tibial osteotomy patients including:
- knee joint line orientation,
- medial proximal tibial angle
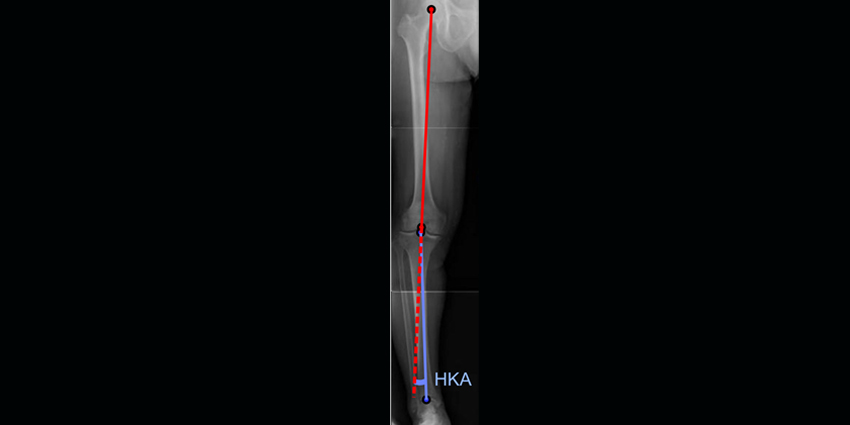
- hip–knee angle
- mechanical lateral distal femoral angle
- lateral distal tibial angle
- knee joint line congruence angle
- ankle joint line congruence angle
- ankle joint line orientation
The team then introduced four additional radiographic parameters which would measure knee and foot positioning by way of a long-leg X-ray including:
- malleolar distance to midline
- intermalleolar distance
- condylar distance to midline
- and intercondylar distance
While, as Dr. Bartholomeeusen acknowledged to OTW, the ensueing process was a bit more theoretical than clinical, it still allowed him and the team to come up with, as he put it, “A simplification of the changes in lower limb alignment in two steps (as described in the article) correction and the adaptation step.”
“The simplification of this process showed me that the foot and knee position after high tibial osteotomy are both crucial to describe the adaptation of the lower limb and thus the changes of knee joint line orientation after high tibial osteotomy. Subsequently I used our radiographic database to test this theory and I was able to confirm the important influence of foot and knee position to knee joint line orientation changes after high tibial osteotomy.”
Why this is a particularly important study?
What makes this particular study so interesting and important, we think, is that, as Dr. Bartholomeeusen explains, it resulted in a new proposed theoretical model of correction and the type of patient adaptation after high tibial osteotomy surgery and, further, the way in which this research team confirmed this new theoretical model with clinical data.
Dr. Bartholomeeusen: “The introduction of foot and knee position and the fact that these are not always the same after re-alignment surgery is also important, again because it changes the way we should look at our patients after these procedures.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.