Outpatient surgeries are often touted for offering equal and in some cases better results as inpatient procedures. In the case of surgical fixation of isolated ankle fracture, outpatient safety data has been limited until now.
Treating Ankle Fractures as an Outpatient Procedure
1 min read Premium comments
#anklefracture#outpatientsurgerySecondary#inpatient#surgicalfixationofisolatedanklefracture
According to a new study, “Outpatient Versus Inpatient Surgical Fixation of Isolated Ankle Fractures: An Analysis of 90-Day Complications, Readmissions, and Costs,” recently published in May-June 2020 issue of The Journal of Foot & Ankle Surgery, for select patients, outpatient surgery to fix an ankle fracture can be safe and more cost-effective.
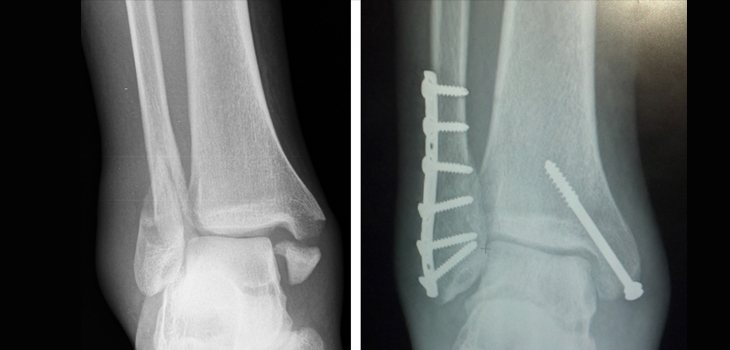
The researchers created an outpatient and inpatient cohort from the 2007 to 2014 Humana Administrative Claims Database. All patients had undergone open reduction internal fixation for unimalleolar, bimalleolar, or trimallelolar isolated closed ankle fractures.
Both cohorts were matched by age, sex, race, region, fracture type and Elixhauser Comorbidity Index. Overall, there were a total of 5,317 inpatient-treated and 6,941 outpatient-treat closed ankle fractures.
The results showed that patients with outpatient ankle fractures compared with inpatient ankle fractures, had lower rate of pneumonia (2.2% vs. 4.0%; p < .001), myocardial infarction (0.9% vs. 1.8%; p =.005), acute renal failure (2.2% vs. 5.3%; p < .001), urinary tract infections (7.4% vs. 12.3%; p < .001), and pressure ulcers (0.9% vs. 2.0%; p = .001).
The outpatient patients also had lower rates of 90-day readmissions (9.7% vs. 14.1%; p < .001) and emergency department visits (13.8% vs. 16.2%; p = .028). In addition, overall 90-day costs for outpatient ankle fractures were nearly $9,000 lower than costs for inpatient ankle fractures ($12,923 vs $21,866; p < .001).
The researchers wrote, “Based on our findings, it appears that outpatient treatment of ankle fractures can be deemed safe and feasible in a select cohort of patients.”
Patients at high risk for complications data shows tend to do better with inpatient surgery where they can be more closely monitored.
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.