The novel coronavirus, technically designated SARS-CoV-2, causes COVID-19 and has tragically been gobbling up global headlines with staggering numbers of new cases and deaths each day. The world is at a standstill with Asia, Europe, and nearly every U.S. state under stay-at-home orders and travel restrictions. Anxiety is spiking as jobs are lost and feelings of isolation set in. Among the headlines are glimmers of hope, indications that regions have passed the peak in new cases or reassurances that social distancing is helping to “flatten the curve.”
Remember Polio? This COVID-19 Pandemic Is Surprisingly Similar
7 min read Premium comments
#covid19#polio#poliomyelitis
Typically, expert commentators have been comparing COVID-19 to Ebola, SARS, or MERS outbreaks, as well as the Spanish Flu from over a century ago. Few are few alive today who lived during the 1918-1919 Spanish Flu pandemic.
There was, however, a more recent global epidemic that struck fear across the world, seemed unstoppable in its ability to strike anyone down. During the 1930s, 40s and 50s Americans feared poliomyelitis with the same kind of deep, visceral anxiety that they fear COVID-19. Like COVID-19, poliomyelitis seemed to strike down children, mostly, but also adults (Franklin D. Roosevelt) seemingly at random. Like COVID-19, polio was relentless, unmerciful and the only solution, aside from isolation, was a desperate race for a vaccine.
Polio
Poliomyelitis is the disease caused by the three strains of the poliovirus and can cause paralysis in severe cases. Approximately 24% of infections cause symptoms of poliomyelitis, and 1% of infections result in acute flaccid paralysis. Few treatments existed to relieve the symptoms of poliomyelitis, such as bed rest, and pain management. The poliovirus attacked the nervous system, and in the worst cases the virus affected the brainstem resulting in paralysis of the muscles in the chest, such as the diaphragm, prevented children from breathing on their own. The inability to breathe independently resulted in the death of 5-10% of paralytic patients.
Physical therapy was important to prevent deformities due to muscle loss in less severe cases. The device most closely associated with the severe effects of polio was the tank respirator, also known as the iron lung. The iron lung, in the 1930s, cost as much as $1,500 (nearly $24,000 today) and was equivalent to the cost of a home at the time. Due to the size and cost of the units, the early mechanical ventilators were often in short supply. During the peak of the epidemic hospitals increased their supply of iron lungs, removed walls, and installed wards full of iron lungs to support the afflicted children.
Paralytic poliomyelitis virus peaked at over 21,000 cases in 1952. Poliovirus typically infects young children, as adults in the 1950s were likely to have been exposed as children. We now know that changing hygienic standards were a contributing factor in the surge of poliomyelitis cases. Children who were exposed to less hygienic environments were observed to have a lower incidence of poliomyelitis during the epidemic.
Social Distancing in the 1950s
Not having a cure or preventative for polio and not really the source of the virus or understanding how it moved through the population, led Americans to practice social distancing; swimming pools, theaters, churches, and schools were closed in attempt to stymie spread of the disease.
The Desperate Search for a Vaccine
Here is where the parallels with Polio and COVID-19 appear so strong.
Resources were poured into various labs around the country to try to find a cure or preventative for polio.
The two lead laboratories were under Jonas Salk and Albert Sabin.
We know today that those two labs were both successful and the vaccines they created, tested, and widely produced led to the eradication paralytic poliomyelitis by 1979 in the U.S., and the western hemisphere by 1994. Most of the world is now polio-free.
Jonas Salk’s Vaccine and Clinical Study
Jonas Salk’s lab was backed by the National Foundation for Infantile Paralysis (NFIP), also known as the March of Dimes. He was focused on a vaccine based on dead polio virus. With the help of multiple public institutions and private corporations Salk’s team was able to produce enough virus to supply vaccine for an historic clinical trial.
The trial was designed with two arms to account for biases in the population that could throw off the results if only those who received the injection were volunteers. The first arm of the study was to inject the dead virus into second graders whose parents volunteered, while first and third graders at the same schools were simply observed.
Why this approach? The panic among parents at the time was so strong that Salk and his team worried that more affluent families would somehow buy their way into the study and bias the results against the vaccine, as affluent children were afflicted disproportionately.
The second arm was a randomized, placebo-controlled study that effectively nullified the bias. Concerns over the ethics of not providing a vaccine were aired, but the trial was carried out regardless.
Incredibly, 600,000 children were injected with vaccine or placebo, and over 1 million were observed. Results were released in 1955. It was broadcast live across the county in cinemas where as many as 50,000 doctors watched. The data showed that Salk’s vaccine, using a dead virus, was 80-90% effective. It was licensed the following day. Salk’s vaccine went on to virtually eliminate cases of polio in the following years. Unfortunately, a supplier of vaccine, Cutter Laboratories, released a batch of vaccine that was not sufficiently killed and led to multiple cases of poliomyelitis killing five children.
Albert Sabin’s Solution
While Salk was first, Albert Sabin’s approach would ultimately become the dominant form of polio vaccine. In contrast to Salk, Sabin produced an attenuated virus vaccine using a mutated, avirulent strain of polio virus. This vaccine was taken orally and delivered protection from the virus for much longer than the injected Salk vaccine, and had less risk of causing polio.
The Amazing Parallels Between the Polio Virus and the Corona Virus
Orthopedics This Week was able to speak with Dr. Paul Anderson, a spine surgeon at the University of Wisconsin Department of Orthopedics and Rehabilitation. Dr. Anderson developed a personal interest in polio after attending a congress of the Brazil Orthopedics Society where he learned of Brazil’s history with the disease and Albert Sabin’s work in the South American country. Dr. Anderson pointed out that modern orthopedics stems largely from work done to help children afflicted by polio. In fact, the word “orthopedics” translates to “straight child.” According to Dr. Anderson there are “lots of parallels about what we’re going through now [with the coronavirus] as with polio when it was active. People did a lot of the same things as now. The polio vaccine was multivalent, it is as yet unclear how a coronavirus vaccine will play out.”
While the poliovirus and coronavirus, and poliomyelitis and COVID-19, are very different symptomatically it is apparent that there are many parallels between the current pandemic and the polio epidemic of the 1930s-1950s. Thankfully, some aspects of the epidemics are different, such as the beneficial impact of social distancing, the rapid development of vaccine candidates, and the relative low-cost and mobility of modern ventilators.
However, it is clear that many concerns are still shared between the two diseases such as the uncertainty of symptom severity, an early a lack of understanding of how the virus affects individuals, and a shortage of critical equipment such as personal protective equipment (PPE), ICU hospital beds, and especially mechanical ventilators.
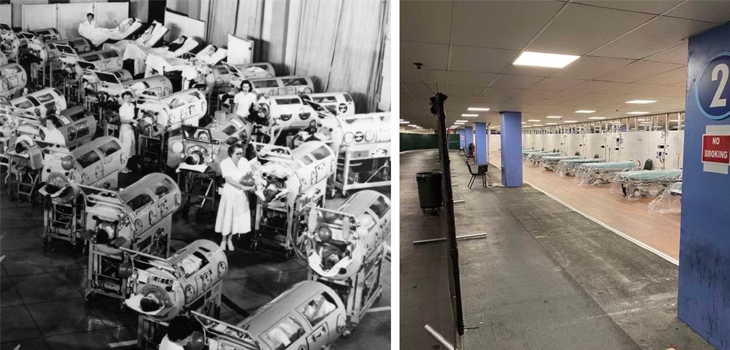
Gymnasiums were converted to house iron lung wards to care for the surge in polio cases, similarly gyms and parking garages have been converted to take overflow patients due to expected COVID-19 cases. The lasting effects of COVID-19 are not well understood either, but permanent lung damage is possible, much like the permanent deformity or paralysis left by poliomyelitis.
The Race to Develop the COVID-19 Vaccine
Due to technological advancements of the last decade vaccine candidates for coronavirus were developed in a matter of hours and days based on sequencing of the viral genome. Despite the rapid identification of potential vaccines, increases in regulation surrounding vaccine development and testing are likely to slow and extend the completion of clinical trials compared to the poliovirus vaccine.
The increased prevalence of coronavirus infection will allow for more robust statistical measurements with smaller populations, and hopefully less time to determine the efficacy. Additionally, positive results, recently announced for antiviral candidates suggest improved outlooks for those most sickened is another positive difference in the response. Such medication was not available for polio, so little could be done but let the virus run its course.
We Have Been Here Before
Hopefully, the coronavirus pandemic will be short-lived and a successful antiviral will soon be approved to reduce symptoms and save lives. Much as it did in the 1950s, a vaccine developed to stop COVID-19 will allow everyone to breathe a sigh of relief and return to more normal activities.
Similar to the polio epidemic, it is likely that everyone alive today will be affected or know someone affected by the disease. We have been here before. And we have prevailed by doing our part and we will do so again, whether it be developing a new drug or vaccine, sewing masks for healthcare workers, or reducing the spread of the disease by staying at home.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.