A team of researchers from the Republic of Korea have come up with a strategy for improving the predictability of ossification of the posterior longitudinal ligament in patients who are conservatively managed. Their work, “How Does Ossification of Posterior Longitudinal Ligament Progress in Conservatively Managed Patients?” appears in the February 15, 2020 edition of Spine.
Link Between Motion and Ossification not so Strong After All
2 min read Premium comments
#cervicalspineSecondary#rangeofmotion#ossificationofposteriorlongitudinalligament
Co-author Dong-Ho Lee, M.D., with the Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine in Seoul, Republic of Korea, explained how the unpredictability of posterior ligament ossification led to this study to OTW, “The background of this article is that it was hard to predict who are at high risk of ossification of the posterior longitudinal ligament (OPLL) progression. Patients with growing OPLL would have increased risk of myelopathy development. If we could predict the ossification of the posterior longitudinal ligament progression using radiographic and demographic factors, and discriminate high risk patients, it would be helpful to set up an individualized follow-up plan.”
“Risk factors which may contribute to ossification of the posterior longitudinal ligament progression for patients who have undergone surgery (laminoplasty) have been reported. However, data regarding patients who did not have surgery remains scarce. And it was not clear whether risk factors and progression pattern that have been reported for postoperative patients could apply to conservatively managed patients.”
In order to improve the clarity surrounding these risk factors, the research team analyzed data from three groups of patients. The first group was comprised of patients with vertical growth >2 mm. The second group were patients whose segments had a thickness progression >1 mm. Finally, those patients who had at least one progressed segment were the third group.
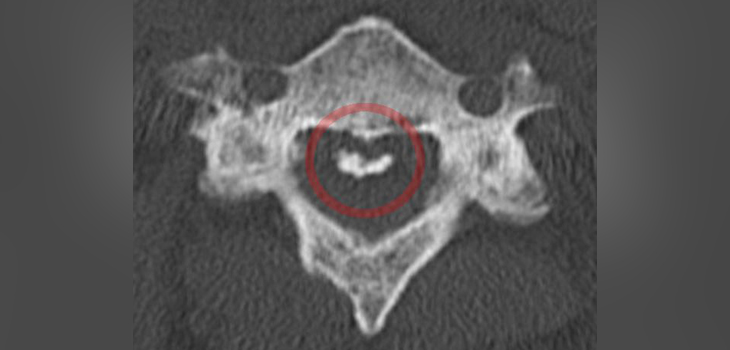
Based on the characteristics at each disc level, the ossified mass at each segment was classified into four types:
- type 1, no disc space involvement;
- type 2, involving the disc space, but not crossing;
- type 3, crossing the disc space, but not fused;
- type 4, completely fused.”
The most important outcome from the study, said Dr. Lee was “A higher range of motion is a risk factor of ossification of the posterior longitudinal ligament progression. Although many surgeons believe that ossification of the posterior longitudinal ligament is associated with range of motion, the data proving the relationship between two factors is limited. As far as we know, this is the first study that proves ossification of the posterior longitudinal ligament growth is associated with range of motion in patients who have not undergone a cervical operation.”
“Another important finding is that ossification of the posterior longitudinal ligament growth is associated with morphology of ossification mass that involves the motion segment. According to our study, ossification mass morphology of ‘crossing the segment but not completely fusing (type 3)’ was associated with high risk of progression.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.