Researchers from Imperial College London and The Royal College of Surgeons in Ireland set out to test a low-cost patient-specific instrument (PSI) design.
No Robot Required When Using Patient-Specific Instruments?
2 min read Premium comments
Secondary#unicompartmentalkneearthroplasty#mako#acrobot
Their work, “A novel patient-specific instrument design can deliver robotic level accuracy in unicompartmental knee arthroplasty,” was published in the September 10, 2019 edition of The Knee.
Co-author Justin P. Cobb, M.Ch.(Oxon) is chair, Section of Orthopaedics at the MSk Lab at Imperial College London. He commented to OTW, “We developed this approach based on our earlier robotic experience, which convincingly demonstrated that accuracy improved outcomes, based upon plans made from CT—something that we had been doing for a long time—since the first trials of the Acrobot—the predecessor of the Mako robot—back in the last century.”
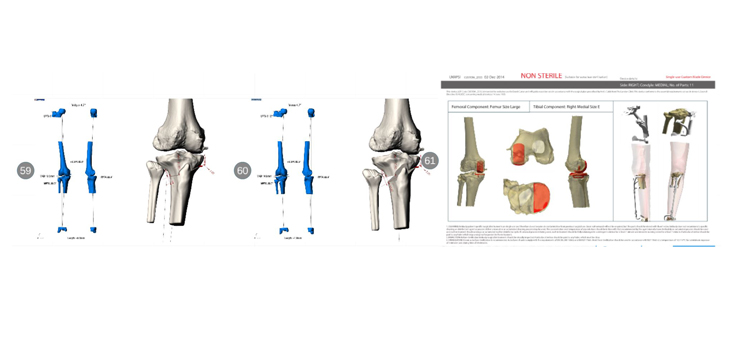
Working with 30 patients who underwent medial unicompartmental knee arthroplasty (UKA), the researchers planned the tibial component position with a CT scan and compared it to a postop day one CT scan to assess the difference between the planned and achieved positions.
Dr. Cobb told OTW, “What was novel was the automation code that Susannah Clarke, Ph.D. and her team wrote which took the plan and the bones, and automatically created the guide shapes, which are then printed in nylon. These guides use several elements which ensure that the operation is performed with robotic level accuracy.”
The authors wrote, “The mean absolute difference between planned and achieved tibial implant positions using PSI was 2.0° in the coronal plane, 2.8° in the sagittal plane, and 4.5° in the axial plane. These results were not significantly different to the 13 historical robotic cases. PSI mean operating time was on average 62 min shorter than the robotic group and 40 min shorter than the conventional instrument group. No complications were reported.”
Dr. Cobb noted, “The use of 3D printing technology also allows us to plan procedures of a complexity that the current robotic platforms cannot match, and then print the instruments needed to enable the procedure to be performed—a corrective osteotomy (undoing an osteotomy that was done years earlier making the joint unstable, and a partial knee at the same sitting for instance.”
“While robotic systems are excellent, they are limited by the procedures in the robotic software.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.