More than 500 patients have been treated with the newly FDA approved Barricaid annular closure device—in Europe.
Finally, Annular Closure Is Being Used in the U.S., Again
2 min read Premium comments
#barricaid#intrinsictherapeuticsSecondary#discectomy
Manufactured by Woburn, Massachusetts-based Intrinsic Therapeutics, Barricaid was tested in a European multicenter, randomized controlled trial involving 554 patients. The study outcomes led investigators to conclude that using Barricaid reduced the rate of recurrent symptomatic herniation by approximately 50% when compared to patients treated with discectomy alone.
The inaugural U.S. implant was performed by New York University’s Langone Health Center to repair a large annular defect. Jonathan R. Stieber, M.D., clinical assistant professor in the Department of Orthopedic Surgery, and Michael L. Smith, M.D., assistant professor in the Department of Neurosurgery and neurosurgeon at NYU Langone’s Spine Center, performed the initial procedure.
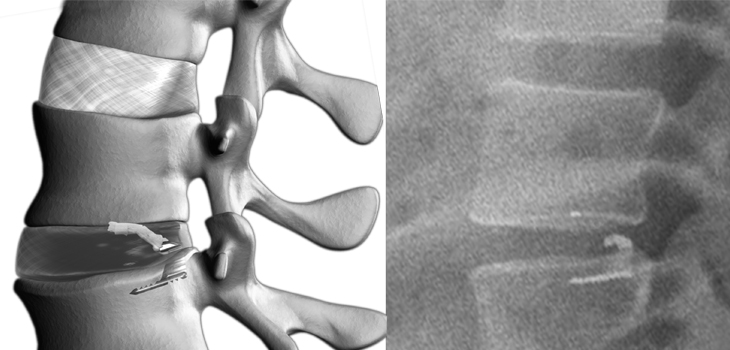
Barricaid is a titanium bone-anchored and polyester implant and is indicated for patients undergoing discectomy who suffer from radiculopathy and back pain due to herniated disc in the lower back.
“We’re excited to be the first in the United States to perform discectomy with implantation of the Barricaid, addressing what has been a long unmet need in the field of spine surgery,” says Dr. Stieber. “While the current standard of care—discectomy alone—is safe and effective to surgically remove the herniated disc material, we have not yet had a reliable way to avoid reherniation in a certain high-risk population.”
“We determine during surgery if the patient has an annular defect that could benefit from repair,” says Dr. Smith. “Implanting the Barricaid device is then immediately performed following the discectomy. The patient should be able to go home after a few hours in the recovery room.”
“This milestone in spinal surgery procedures demonstrates NYU Langone’s commitment to creating the best outcomes for our patients by adopting innovative techniques that are supported by peer-reviewed published evidence,” says Joseph D. Zuckerman, M.D., the Walter A.L. Thompson Professor of Orthopedic Surgery and Chair of the Department of Orthopedic Surgery. “Our use of cutting-edge treatments serves to both advance the field of orthopedic surgery and improve the quality of life of our patients by reducing their pain, and their risk of re-hospitalization and additional surgery.”
Dr. Jonathan Stieber told OTW, “Sizing and insertion of the device is straightforward and similar to implantation of other interbody devices. Specific attention must be paid to the angle of insertion in order to properly seat the titanium anchor.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.