The team from the University of Toledo, Ohio—led by legendary Orthopedic and Spine researchers Aakash Agarwal, Ph.D.—has published a retrospective study which makes a case that active apex correction (APC) may reduce the risk of correction loss while a child is growing and therefore, preclude the need for repeated surgeries using traditional growth rods for children suffering from spinal deformity.
Apex Correction a Superior Deformity Approach?
6 min read Premium comments
#apex#shilla#vertebralremodulation
Researchers Highlight Benefits of Modified SHILLA Technique
Aakash Agarwal, Ph.D., and his great team of scientists—Loai Aker, M.D. and Alaaedldin Azmi Ahmad, M.D. of Annajah Medical School in Palestine—followed 20 pediatric patients under the age of 8 who were undergoing surgery for spinal deformity—specifically for scoliosis or kyphoscoliosis. The results were published in Global Spine Journal and the team presented follow-up data comparing this technique and traditional growth rods in Spine Surgery and Research.
What did the study show? Simply put, APC may be preferable to promote growth guidance over the traditional SHILLA™ technique, which is currently one of the standard surgical approaches.
When asked about what sparked interest in pursuing this research, Agarwal explained to OTW, “The impetus came from the work of Dr. Alaaedldin Azmi Ahmad, who, in trying to control severe type 1 congenital kyphosis in the thoracolumbar region of children with early onset scoliosis, used a technique which involved putting screws above and below the peaked wedged vertebrae in association with growth rods. After more than 2 years of follow up for 13 patients, he realized that the wedging of the peaked wedged vertebrae dramatically improved.”
Longer Lasting Correction as Children Grow, Fewer Repeat Surgeries
Agarwal and his colleagues explained that using the traditional SHILLA procedure frequently leads to loss of correction due to crankshafting or adding-on. Such phenomenon occurs as the child grows and can result in either return of deformity or loss of the correction previously provided by SHILLA. In addition, traditional SHILLA requires fusion at the apex, and there exists a significant risk of complications due to need for osteotomies on the concave side.
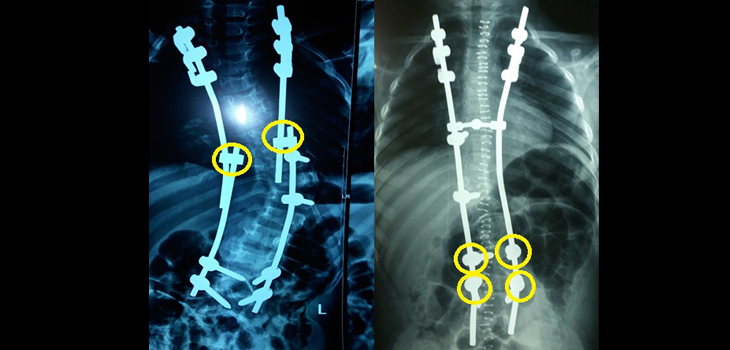
So, the team looked at a modified non-fusion SHILLA procedure, active apex correction (APC) which involves placing pedicle screws both above and below wedged vertebra, on the convex side. In this manner, compensatory pressure can be created on the vertebra via compression of pedicle screws before tightening. This allows for reverse modulation and over time, wedging reduction. It can also provide a foundation for growth guidance at the apex of the curvature.
Importantly, the technique avoided osteotomies and no screws were used on the concave side of the apex. In fact, it only required 2 screws at the apex of the curve, as opposed to 6 screws which are typically used in traditional SHILLA surgery.
Fewer screws, lower cost.
Also, a better outcome?
Employing this approach, Agarwal, Aker and Ahmad, found that the wedging at the apex was substantially reduced.
It is well described in the literature that loss of correction in traditional SHILLA is linked to the inability of the apical fusion to halt progression of deformity as a child grows. With the APC approach, the ability to substantially reduce apical wedging provides a tool to mitigate such occurrences.
As Agarwal and colleagues explained to OTW, “The result of this study provides clinical evidence of reverse vertebral modulation at the apex of the curve in patients with scoliosis and kyphoscoliosis, when modifying the traditional SHILLA technique with APC.”
The researchers also compared this technique with traditional growth rods, which are commonly used in developing countries; in contrast developed countries have completely transitioned into magnetically controlled growth rods. A major problem with traditional growth rod technique is that it requires repeated invasive surgeries to distract the spine.
The researchers demonstrated equivalent clinical results between APC and growth rods, without the need for repeated surgeries with the latter, thus recommending it as a safer substitute to traditional growth rods.
A Closer Look at Methodology
The hospital’s institutional review board approved the 6-year study. The investigators enrolled 20 children who they’d diagnosed with scoliosis and kyphoscoliosis and were scheduled to undergo either index surgery or revision surgery. According to the study researchers, each patient’s imaging showed “clear evidence of vertebral wedging at the apex.” The investigators also included a subgroup of children with congenital disease. Finally, the researchers noted that the patients they’d enrolled presented with malformation, malsegmentation and unilateral bony bar.
The study authors acknowledged the limitations of their study, including the number of patients and the fact that the precise amounts of applied compression at the apex was not measured.
The researchers performed all of the pediatric spinal surgeries with an intraoperative neuromonitor and C-arm. In the modified SHILLA version of the study, the researchers used Medtronic’s SHILLA screws. When these screws were not available, they used rod to domino sliding.
The authors selected the most severely wedged vertebra, and inserted pedicle screws into the convex side of the vertebrae both above and below the noted wedged vertebra. They did not insert any screws on the concave side of the apex.
The researchers primarily used an extraperiosteal technique, with the exception of the convex side of the apical/wedged vertebrae. The authors placed screws at this site for compression and placed rods and domino subfascially to avoid prominence.
The researchers used computed tomography to measure the convex and concave heights of wedged vertebrae at the time of surgery and at follow up.
Finally, the investigators chose patient-specific control vertebra with similar physical dimensions to the wedged vertebra to record standard growth rates for the duration of follow up and the age of each patient. They did not apply compression forces at the convex end of the control vertebra.
The patients did not use post-operative casts or braces. The average duration of follow-up was 32 months; 8 months was the minimum.
Results
In their first study (published in GSJ), the authors reported that “The wedged vertebra demonstrated an average increase of 17% (P =.00014) in the proportion of concave to convex heights ratio” and that “as expected, the control vertebra did not show any lateral deviance in the heights at the follow-ups.”
Agarwal and colleagues concluded that, “APC, instead of apical fusion in SHILLA, remodulates the apex vertebra, which may in turn help mitigate the loss of correction on long term due to crankshafting and adding on.” This may also translate into less invasive surgical procedure for children struggling with spinal deformities.
In their second study (published in SSRR), the researchers stated, “In conclusion, the results of this study suggest clinical equivalency with respect to correction, between the two clinical procedures, APC and traditional growth rod systems, at the current follow up period, however the latter presents an obvious disadvantage because it requires multiple surgeries to regularly distract the spine.” In this study they showed in countries with limited resources, where traditional growth rods are widely used, could instead benefit from APC. An equivalent method which requires fewer surgeries may translate into less pain, better recovery time and medical follow-up for such children and their families.
Looking Forward
Agarwal and colleagues will continue to conduct research and educate about this very interesting and novel approach. They are committed to improving surgical treatments for scoliosis and kyphoscoliosis.
Agarwal told OTW, “We would like for the deformity surgeons across the globe, who currently are using either conventional SHILLA technique and are experiencing crankshafting/adding-on/distal migration or traditional growth rods (repeated invasive surgery because patients can’t afford non-invasive magnetic growth rods), to try this technique (and publish their two, five, and ten years of follow-up results).”
Agarwal continued, “Essentially this technique is a hybrid of two key concepts: tethering/stapling (active in nature) and growth guidance (passive in nature).”
“Lately our team has been thinking about adding a third concept: distraction on the concave side (to improve the remodulation intensity), but we are still working on that concept with Professors Anand Agarwal, Arvind Jayaswal, and Vijay Goel. Perhaps we can incorporate another upcoming method called SDS (Spring Distraction System) into it, invented by Professors Rene Castelein and Moyo Kruyt. Traditional growth rods surgery is obsolete and more traumatic than other contemporary techniques, and it’s high time we let it go!”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.