“No labral repair for you,” is what many patients over the age of 60 have heard. But is that really the best approach?
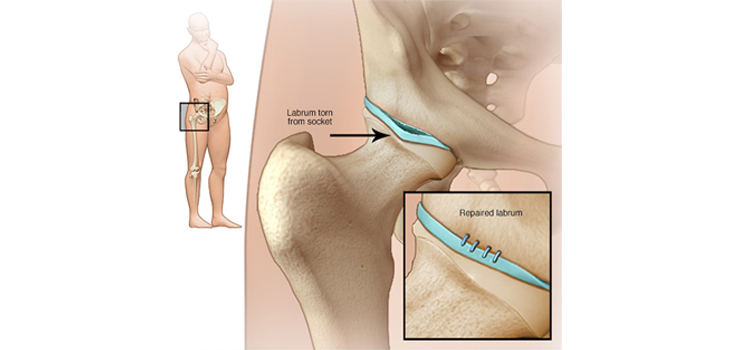
Acetabular Labral Repair: Patients 60+ Fare Well Too?
2 min read Premium comments
Secondary#femoracetabularimpingement#acetabularlabralrepair
A team of researchers from Tennessee decided to find out. Their work, “Arthroscopic Acetabular Labral Repair in Patients Over the Age of 60 Years: A Matched Case-Control Study,” appears in the May 2019 edition of Arthroscopy.
J.W. Thomas Byrd, M.D., orthopedic surgeon with the Nashville Hip Institute and study co-author explained the genesis of the study to OTW, “Over several decades in our practice, we observed the positive results associated with the evolution in acetabular labral treatment from debridement to repair.”
“This was based on four factors:
- The healing capacity of the labrum was established;
- The technique for labral repair was refined;
- Technical advancements in anchors and suturing devises were readily available; and
- The rehab strategies were streamlined making the recovery process less onerous.”
“We have seen no reason to deny the value of labral repair to older patients.”
“Numerous published studies suggest that older patients are not good candidates for arthroscopy; but that is simply not the case. Almost a decade ago when we published our prospective analysis of hip arthroscopy with 10-year follow-up, we showed that older patients didn’t do as well, only because they had more associated problems with arthritis.”
“When we excluded those with significant arthritis, older patients did just as well as younger patients. Arthritis is bad regardless of age. Arthroscopically, arthritis is gauged by the severity of articular damage.”
For their study, Dr. Byrd and his colleagues looked at patients whose average age was 63.2 years. Twenty of the patients in the study were diagnosed with femoroacetabular impingement whereas 1 was diagnosed with dysplasia. According to the research team, “Of these patients, 19 had acetabular articular damage (grade IV in 2, grade III in 11, grade II in 5, and grade I in 1) and 6 had femoral changes (grade IV in 1 and grade III in 5).”
“The results of labral repair in patients over the age of 60 are just as good as younger adults when matched for the severity of associated articular damage. Poor results and likelihood of conversion to total hip arthroplasty were associated with combined Outerbridge grade III & IV damage to both the acetabular and femoral surfaces. This observation is true for both the study and control groups,” said, Dr. Byrd.
“Severe associated articular damage may be a contraindication regardless of age. However, there remain numerous and various other factors that influence the decision about surgery in each individual.”
“How clearly is the identified pathology affecting the individual’s life? What are the patient’s desires and motivations towards their own recovery? Are they otherwise reasonable candidates for hip arthroscopy regardless of how you manage the labrum?”
“Do not use this data as an excuse to recommend surgery for every MRI-reported labral tear, which can often be the normal consequence of aging. But it can be appropriate to offer older patients the option of labral repair if they are otherwise a candidate for hip arthroscopy; and you don’t have to just tell them that they are too old to fix their labrum.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.