When we last heard from Intrinsic Therapeutics, Inc.’s Cary Hagan and Greg Lambrecht it was December 12, 2017 and the FDA Orthopaedic Advisory Panel had just voted against recommending approval for the company’s Barricaid Anular Closure Device (ACD).
The Rough Road to FDA Approval for Barricaid Anular Closure Device
6 min read Premium comments
#intrinsictherapeutics#fda#discherniation
The FDA Panel yielded a nearly unanimous vote on effectiveness of the device, but had concern over specific safety questions regarding endplate changes in the disc.
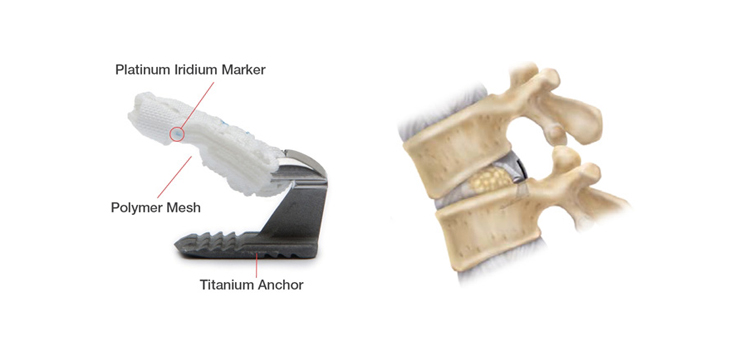
The device is designed to close large defects in the anulus to prevent recurrent disc herniation, while allowing the surgeon to preserve more of the patient’s disc. It consists of a woven polyester occlusion component intended to block an anular defect, while anchored to the adjacent vertebral body by a titanium bone anchor.
The Panel didn’t see all the data and we reported at the time that we thought the panel had missed the forest for the trees.
Apparently, the FDA scientists agreed and granted premarket approval (PMA) for the device on February 8, 2019.
More on the technical details later in this story. The interesting story is how the company reacted.
Off the Mat
Intrinsic is a start-up company with one product. When the panel of orthopedic experts vote against approval of that product, you either die or try to pick up the pieces.
Hagan said the company employees were devastated following the panel vote. They bucked up for a rough ride and laid off nearly a third of their staff. Hagan credits the investors for staying steady in the turmoil and is proud that not one single member of the remaining staff bailed out. He said the commitment from the staff was due to their unwavering belief that this product made a significant difference in the trajectory of patients’ lives.
The PMA route to FDA blessing is the toughest way to go, requiring an IDE (investigational device exemption) pivotal clinical trial. Most devices get to market via the less expensive, much faster and easier 510(k) clearance route where you only have to show your device is substantially equivalent to a previously approved or cleared product. As a result of the time and expense involved, PMAs are very rare.
But Intrinsic’s novel anular closure device was so different from anything else in the market that there was no previous device predicate to make a determination of safety and effectiveness. Hagan said in preliminary discussions with FDA staff they considered anular closure a Class 1 device, requiring a PMA rather than the much simpler and quicker 510(k) pathway.
Superiority
The Intrinsic team made another tough decision in the preliminary stages of discussions with FDA staff. They would do something very few companies do when following the PMA path. Most companies set out show “non-inferiority” to existing gold standard devices. The crew at Intrinsic were so convinced of their data, they decided to prove clinical Superiority to existing treatments.
Hagan admits he had some trepidation with that extra difficult approach, but the huge gamble on a Superiority trial was worth the risk.
In the midst of the devastating panel vote, Hagen said the data on Safety, Efficacy and Benefit-Risk was far too compelling to consider throwing-in the towel.
The Panel Meeting
The company ran out of time during the Panel meeting to answer all the questions posed by Panel members and FDA staff. With unanswered questions, there was still a path forward.
Hagan said there were approximately 50 of those questions from the Panel that remained unanswered at the time that the Panel was asked to vote. “In retrospect,” Hagan told us, “we simply ran out of time to share the data that had been carefully prepared to answer the Panel questions. The data and slides were ready to share, there was simply no opportunity to respond.”
The subsequent questions posed by FDA gave the company an opportunity to present more evidence regarding safety. For instance, the company was able to provide data from 334 additional patient time points which showed a 50% treatment differential between the Barricaid group and the control group.
“Fifty percent is a high number, especially considering the high rates of reherniation and treatment costs of patients who have to go back for second, third and even fourth surgeries,” said Hagan.
Through a patient and consistent interaction with FDA staff, Intrinsic and the team at MCRA (Musculoskeletal Clinical & Regulatory Associates) built a successful case for safety. In the end, the FDA staff saw the forest for the trees.
Lessons
We asked Hagan what lessons he took away from this FDA experience and what advice would he give his colleagues who may experience the same thing in the future.
First, said Hagan, “listen actively to the questions posed by FDA staff.”
Second, “take extra time with the FDA review team to clarify and confirm exactly what they want and what they think they are hearing from you.”
And finally, “Be patient. Very patient.”
“I have a positive view of FDA,” said Hagan. “Other than the time limitation of the Panel meeting, this process worked like it is supposed to work. The FDA worked very hard, spent huge amounts of time and were extremely responsive in the scientific process. It was extremely difficult and cost us one year, but it was fair.”
The Evidence
Before we close this happy story, let’s look at the safety issues Hagan and his team had to patiently address with the Panel and FDA staff.
According to the FDA approval document, the device is “indicated for reducing the incidence of reherniation, and reoperation in skeletally mature patients with radiculopathy (with or without back pain) attributed to a posterior or posterolateral herniation, and confirmed by history, physical examination and imaging studies which demonstrate neural compression using MRI to treat a large anular defect (between 4-6 mm tall and between 6-10 mm wide) following a primary discectomy procedure (excision of herniated intervertebral disc) at a single level between L4 and S1.” Lumbar discectomy is considered to be the largest unaddressed market in spine.
The FDA Panel voted 9-5 against recommending approval due to safety concerns. The Panel members’ safety concerns stemmed from the FDA staff noting to members that CT imaging showed bone changes to the vertebral endplates for some of the Barricaid patients.
Eighty-eight percent of the patients receiving Barricaid had endplate changes versus 40% of control patients. The control patient’s changes were slightly smaller on average and appeared to stabilize sooner than the Barricaid patients. The Barricaid endplate changes were larger and had a distinctive radiographic feature—according to the FDA’s radiologist.
But when Hagan and team were able to address all the leftover questions from the panel meeting, they were able to show that endplate change stabilize and that the use of Barricaid cut recurrent disc herniations, re-operations and serious adverse events by roughly 50%, a difference that was highly statistically significant. “These measures,” added Hagan, “clearly have a meaningful impact on patient quality of life.”
Cost Savings
Beyond a meaningful impact on patient quality of life, there is a significant impact on the patient’s (or their insurer’s) pocketbook.
As we reported after the Panel meeting, among the data not presented to the Panel was a health economics analysis—which looked squarely at the issues of re-herniation and a higher rate of adverse events when NO annular closure device is used.
An independent economist conducted the analysis using two-year follow up data from the Barricaid RCT study. Here is a summary of the findings.
Barricaid’s QALY (quality-adjusted life year) score was $6,826 versus $76,023 for conventional lumbar discectomy
After performing 1,000 simulations as part of a sensitivity analysis, 93.3% of the simulation results were below the $100,000 Willingness-to-Pay threshold.
According to an Intrinsic write-up:
“Most of the cost savings—approximately 85%—came from the reduction of reoperations due to the reduction in reherniations. The majority of the remaining 15% of the cost savings came from lower rates rehospitalizations (due to fewer SAEs). Lower rates of reoperation mean fewer diagnostic tests, less physical therapy, and reduced medication.”
In health economic terms, this kind of data represents dominance over conventional lumbar discectomy—where, as the economist described it to OTW, “dominance” is defined as when a procedure is both more efficacious and cheaper than the alternative—“you get more for less.”
Hagan and his team took the tough road and almost became roadkill. But perseverance, steady investors and unassailable evidence kept this device alive and will help a lot of patients.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.