That legislation aimed at dealing with the opioid crisis (“Opioids Bill Means Sweeping Changes to Pain Management,” Orthopedics This Week, Wednesday, October 10, 2018) was signed into law by President Trump on October 24, as expected.
Trump Signs Opioids Bill – Here’s What to Expect
5 min read Premium comments
#painmanagement#opioid#opioidlegislation
By one measure—its length, at 660 pages—it’s probably the biggest federal opioids law ever written. In terms of effects on the practice of medicine, it’s important, but more for its potential to inflict pain on caregivers than for any other reason. (The story cited and linked above describes its key provisions affecting orthopedists.)
As for the likely effects of this hodgepodge of legislative initiatives on the opioid crisis, it’ll probably help a bit, but not much, considering what is already happening.
- The Centers for Disease Control (CDC) 2016 guideline on opioid prescribing seems to have had a major impact. Vast numbers of physicians have taken it to be a de facto It has been widely criticized as insufficiently case-specific, and both the CDC and Food and Drug Administration (FDA) have announced plans to issue more detailed, evidence-based guidelines (“Are FDA and CDC at War Over Opioid Regulation?” Orthopedics this Week, October 8, 2018), but caregivers are clearly paying attention to the guideline.
- Stepping well beyond guidelines, states have taken the lead in passing laws limiting durations and/or strength of opioid prescriptions. In all, 33 had enacted such laws by September, according to this National Conference of State Legislatures report and this September 2018 follow-up, both by analyst Kate Blackman.
- All 50 states now have prescription drug management programs (PDMPs), most of which require physicians to check a patient’s prior opioid meds while writing prescriptions (“Are Ortho Prescription Drug Monitoring Programs Working?”, Orthopedics This Week, August 8, 2018). PDMPs make it more work to prescribe an opioid. They also have a Big-Brother chilling effect, in that federal and state drug enforcement snoop through that PDMP data to catch prescribing abuses and pharmacy dispensing abuses of opioids.
- Under legislation passed in the Obama years, the National Institutes of Health are already offering grants to find new alternatives to opioids for managing pain. This might well prove to be the most important single non-law-enforcement step in the long run, if affordable alternatives can be found.
- As of early 2018, Medicaid was already covering at least one opioid abuse treatment in 49 states, and most covered all three main-line treatments, according to a Kaiser Family Fund report. Prescriptions for opioid treatment have skyrocketed.
- Also, not waiting for the new law, the Centers for Medicare and Medicaid Services (CMS) proposed extra reimbursement for the analgesic Exparel to expand its use as a postoperative alternative to opioids for total knee arthroplasty at ambulatory surgery centers. CMS asked for comment on whether to offer that reimbursement boost to hospitals and to use of Exparel for other surgeries, and to other opioid alternatives (“CMS to Pay Extra for Exparel in ASCs, Not Hospitals,” Orthopedics This Week, October 9, 2018).
- With all the pressures listed above and others, opioid prescribing was down 29% from its peak in 2011 to the end of 2017, an April 2018 IQVIA report A recent CDC study using the IQVIA data came to a closely similar conclusion, saying prescriptions peaked in 2012, and fell 27.8% from then through 2017. IQVIA said the biggest declines in prescribing were from 2015 to 2016, and then a still steeper decline from 2016 to 2017. That trend seems to suggest that the decline in prescriptions continues, and might even be accelerating, in 2018 in advance of any effects of the new law. “These numbers don’t tell you what exactly is driving the acceleration in the drop, but we think it’s useful to get the 2017 numbers out there so people can see what’s happening,” Murray Aitken, executive director of the IQVIA Institute, told The New York Timesin an April interview.
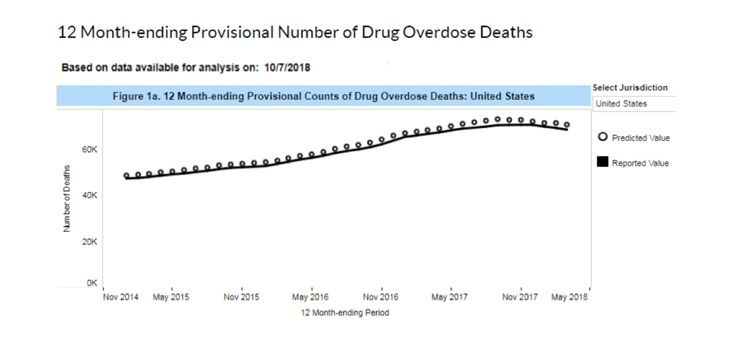
- New, incomplete, “provisional” CDC data indicates that overall, opioid deaths nationwide started to decline slowly in about December 2016, and continue to do so for the latest period in which statistics are available.
The new law was rushed through Congress to answer a political need. U.S. Senate and House incumbents of both parties who are running to keep their seats can point to its sheer mass when they’re asked, “What are you doing about the opioid crisis?”
The bill was created in early autumn by quickly mashing together, in time for the midterm campaign season, more than two dozen smaller bills which had been introduced separately. It was sent to the floor of the Senate and House without the lengthy research and hearing period which normally precede legislation of its scope.
Evidence for the view that this law was at least in part aimed at the upcoming midterm election: As of September 19, political ads mentioning opioids had run more than 50,000 times in races for Congress and governor in 25 states. In 2014, by comparison, there’d been just one opioids political ad, in Kentucky, which aired 70 times, according to an analysis by The Wall Street Journal.
The law “is everything but the kitchen sink,” Daniel Ciccarone, M.D., M.P.H., a professor of family and community medicine at the University of California at San Francisco, is quoted as saying in a Washington Poststory on October 24 “Anyone who has any thought about how to address the opioid crisis got a bill in there.”
“I do think it’s woefully underfunded,” said Chinazo Cunningham, M.D., M.S., a professor of medicine at the Albert Einstein College of Medicine and Montefiore Medical Center, in that same Poststory. “It feels to me as though it’s not really a coordinated effort, that it’s bits and pieces—honestly, a little bit working on the edges.”
Further evidence of how politics collides head-on with reality in opioid legislation: former New Jersey Governor Chris Christie bragged in his 2018 farewell address in January that his early 2017 opioid law limiting prescriptions to five days had cut opioid prescriptions by 15% there. Meanwhile, as of October, New Jersey is one of only two states in which opioid deaths will soar more than 15% in 2018 over 2017, according to the provisional CDC data cited above. That projection is based on actual numbers plus a factor for late reporting of deaths for which the cause takes time to determine.
In all, Congress appropriated $8.5 billion for the 2019 fiscal year for opioid programs, but this law doesn’t guarantee any funding for future years.
Again, there’s a detailed roundup of the content of this law affecting orthopedics in our prior news report cited in the lead paragraph above.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.