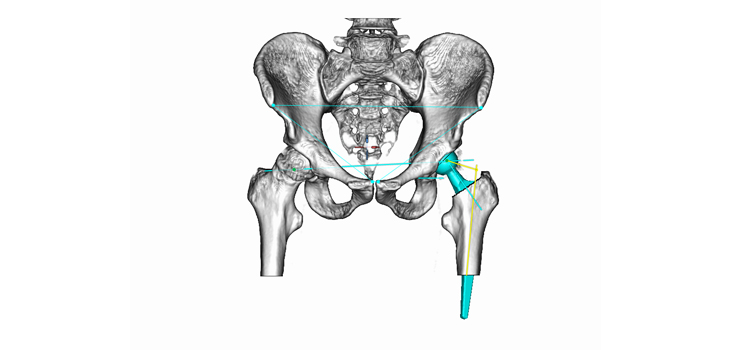
mediCAD Hectec GmbH, based in Landshut, Germany, has launched three preoperative planning tools, mediCAD 4.0 as well as mediCAD Hip 3D and mediCAD Spine 3D.
mediCAD: Preop Planning Tools Launched
1 min read Premium comments
Secondary#medicad#hip#jornseel
According to the company, they have added several new key features that simplify things, including automatic repositioning in the hip planning; automatic recognition of the femur axis when measuring the offset; and a favorites list in the implant database. And surgeons now have the option of placing templates in both AP (anteroposterior) and ML (mediolateral) views simultaneously.
Jörn Seel, CEO at mediCAD Hectec, told OTW, “The process of getting FDA approval is rigorous and can be quite challenging and time-intensive. However, we were already accustomed to working with the FDA on prior approvals of earlier versions of mediCAD. This familiarity with the process and the close cooperation with the FDA staff allowed us to successfully meet the requirements in order to bring this latest version of our software to the orthopedic market in the U.S.”
“mediCAD is the world’s first and most widely used preoperative, digitized planning program for orthopedics. With mediCAD, orthopedic physicians can readily plan surgeries using digital image files of patients scaled to our extensive database of over 130 implant manufacturers’ digitized templates. Using our software, physicians have been able to increase the accuracy of surgical planning and save up to 85% of the time that it previous took for conventional planning using acetate templating. Plus, we are continually working in collaboration with doctors, for doctors, in bringing new products to the market such as 3D planning using CT scans and MRIs and cloud-based planning performed remotely and even from a tablet.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.