On November 5, 2018, the FDA issued a 10-page guidance document which says the agency “does not intend to enforce the direct mark requirements” of the unique device identification (UDI) rule for Class III medical devices that are non-sterile until September 22, 2022.
FDA Pushes UDI Enforcement Back to 2022
1 min read Premium comments
Secondary#foodanddrugadministration#classlllmedicaldevices#uniquedeviceidentificationrule
The agency will delay enforcement for Class III (life-supporting or life-sustaining) devices made and labeled prior to the applicable compliance date if other information of the device can be used to determine the UDI.
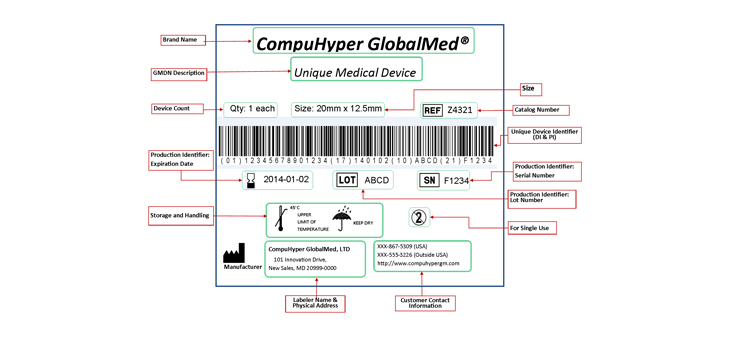
In making that determination, the agency will look for information such as catalog, lot and serial numbers directly marked on the device.
The agency published the original final rule establishing the UDI system on September 24, 2013. The UDI rule required a device to bear an UDI on its label and packages unless an exception or alternative applied.
As the FDA and industry worked to implement the UDI rule, the agency said it identified “complex policy and technical issues that require resolution to help ensure that UDI data are high quality and are available in standardized ways.”
The guidance document notes a challenge for labelers meeting the UDI direct mark requirements for devices finished and labeled before the labeler had achieved direct mark compliance, but which remain in inventory on or after the applicable direct mark compliance date. “The cost of remediating existing devices in inventory to add a direct mark may be substantial, as it can entail different design changes and design validations than those made in order to add a required UDI direct mark to future lots of the device.”
The new guidance supersedes a previous guidance issued on January 16, 2018.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.