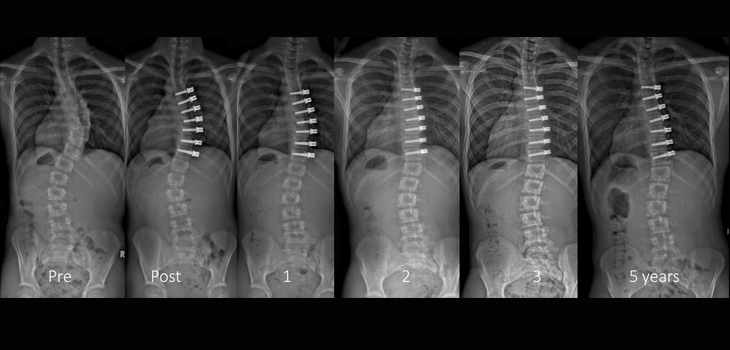
A new retrospective review of 17 patients with thoracic scoliosis who underwent anterior spinal growth tethering (ASGT) has shed light on the subtleties involved in this technique. The study, “Anterior Spinal Growth Tethering for Skeletally Immature Patients with Scoliosis: A Retrospective Look Two to Four Years Postoperatively,” appears in the October 3, 2018 edition of The Journal of Bone and Joint Surgery.
Study: Tethering “Reasonable” in Certain Thoracic Scoliosis Cases
2 min read Premium comments
Secondary#scoliosis#anteriorspinalgrowthtethering#asgt
Co-author Peter O. Newton, M.D., with the department of Orthopaedics at the Rady Children’s Hospital in San Diego, California, told OTW, “Anterior spinal growth tethering is clearly a method that has the potential to correct scoliosis in growing teenagers. I am excited by the promise we may be able to use the remaining growth of an adolescent with substantial scoliosis to result in lasting correction and ultimately avoid a spinal fusion.”
The authors described the study methodology as follows, “Revision surgery was performed in 7 patients: 4 tether removals due to complete correction or overcorrection, 1 lumbar tether added, 1 tether replaced due to breakage, and 1 revised to a posterior spinal fusion. In 3 additional patients, posterior spinal fusion was indicated due to progression. Eight (47%) of the patients had a suspected broken tether. Ten (59%) of the 17 were considered clinically successful.”
Dr. Newton commented to OTW: “The cases presented in this paper demonstrate the challenges as well as the potential of the technique, especially as the follow up gets beyond 2 years. Predicting the effects of a tether over 2-3 years of remaining growth is difficult at present. In addition, it appears our current implants which are being used in a physician directed (off label) manner are not always lasting long enough. The tether is failing, as I believe they all will do eventually, before growth is completed in some cases.”
“Despite these challenges, a spinal fusion has been prevented in the majority of cases. However, the ‘true’ benefit of the retained motion relative to what would have likely been an isolated thoracic fusion can certainly be questioned. The differences in global trunk motion appears to be only modestly affected by a thoracic spinal instrumentation and fusion.”
“There is growing interest in fusion-less treatment for scoliosis. Internet sources and social media in my view often paint a picture praising tethering and damning fusion. This is biased and inaccurate. Patients need clear and balanced information on the pros and cons of tethering vs. fusion. My hope is this paper will offer some of the facts required to inform such discussions.”
“In my view, tethering is reasonable for the growing patient with a scoliosis beyond 45 degrees. They need to understand an attempt to avoid fusion with a growth modulating tether will be less reliable and have a higher revision rate than posterior spinal fusion. Some will value motion over the absolute correction or the greater chance of revision. Others will value the most reliable approach at the expense of a modest loss of motion. Shared decision making is mandatory.”
“I am confident we will be able to create better implants and better predictors of when and how tight these tethers should be placed. In the meantime, we will need to apply the technique judiciously.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.