With all of the patients awaiting an allograft size match, a team of researchers set out to determine if lateral femoral condyle (LFC) grafts could be used to restore the articular surface in patients that require osteochondral allograft transplantation of the medial femoral condyle (MFC).
Criteria for Osteochondral Graft Matching Too Restrictive?
2 min read Premium comments
Secondary
Their study, “Differences in the Radius of Curvature Between Femoral Condyles: Implications for Osteochondral Allograft Matching,” appears in the August 1, 2018 edition of The Journal of Bone and Joint Surgery.
Co-author Peter Du, M.D., a first-year orthopedic resident at the University of Arizona in Tucson, explained to OTW, “With the traditional osteochondral allograft size matching process, patients can often wait anywhere from 6 to 12 months, and sometimes even longer for a donor graft that has size dimensions that are similar to the patient’s knee. Additionally, once a patient is notified of a potential match, we must arrange to perform the surgery within 1-2 weeks before the cellular viability of the graft decreases and the graft is deemed inappropriate for use.”
“Furthermore, there are a number of grafts that ultimately get wasted because they are not able to be used in time. Current data suggests that the overwhelming amount of grafts that are made available to surgeons are LFCs, and the majority of symptomatic lesions that present for potential treatment are MFC lesions. We sought to determine if LFC grafts could be a viable source for accurately restoring the articular surface in patients that require osteochondral allograft transplantation of the MFC.”
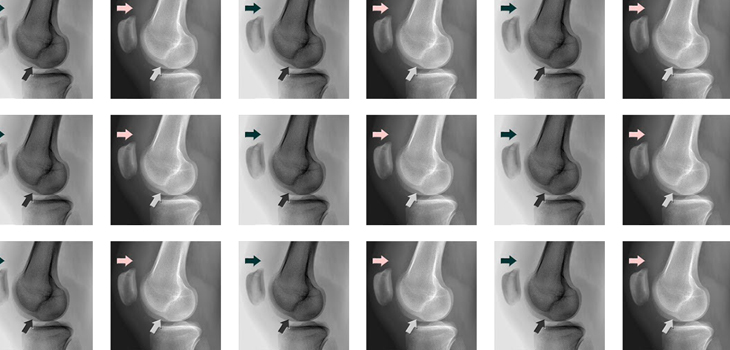
“Only a handful of other studies that have investigated the potential utility of using LFC grafts for MFC cartilage lesions have been performed, and we believed a significant limitation in their study design was the fact that the authors utilized computed tomography (CT) to measure the amount of incongruity observed at the articular surface. We sought to potentially provide more clear data by investigating this clinical question using magnetic resonance imaging (MRI), which is a much more accurate modality for evaluating articular cartilage.”
“We found that 100% of medial to medial transplantations, 98% of lateral to lateral transplantations, and 92.5% of medial to lateral transplantations would be considered acceptable based solely on graft height mismatch criterion (i.e., within 1mm).”
“This seems to suggest that acceptability of donors does not correlate with femoral condylar anterior-posterior lengths or orthoptopic matching of condyles (i.e., using medial donor grafts for medial lesions) and that our current criteria for accepting grafts on behalf of patients may be too restrictive.”
“It appears that we may be able to safely and accurately restore the articular surface by using donor grafts that are not necessarily from the same condyle or precisely the same size as the patient’s condyle in the anteroposterior dimension. We believe it is still important to utilize grafts that have similar size or larger width in the medial-lateral dimension to ensure a sufficiently sized graft can be obtained if the lesion is found to be larger than expected at the time of surgery. In the anteroposterior dimension this problem is less of a concern, because multiple grafts can be stacked in an overlapping configuration to make sure the entire defect is treated.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.