Could stereovision change spine surgery?
Stereoscopic Spine Imaging!
1 min read Premium comments
Secondary#dartmouth#intraoperativestereovisionsystem
A new study, “Stereovision Co-Registration in Image-Guided Spinal Surgery: Accuracy Assessment Using Explanted Porcine Spines,” published in the March 6, 2018 edition of Operative Neurosurgery raises that intriguing possibility.
Co-author and professor of engineering at Dartmouth College in Hanover, New Hampshire, Keith D. Paulsen, M.S., Ph.D., told OTW, “We had developed an intraoperative stereovision system (iSV) for brain surgery and thought it could be applied in spine surgery and eliminate some of the barriers to adoption of image-guidance for spine procedures.”
For their study, the researchers started with 10 explanted porcine spines from which they removed dorsal soft tissue to a variable degree. The team then placed bone screw fiducials in each spine and performed high-resolution computed tomography (CT) scanning.
They then obtained stereoscopic images using a tracked, calibrated stereoscopic camera system.
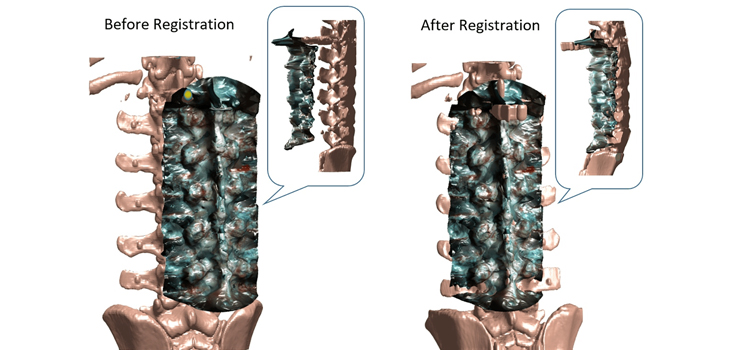
According to the study, “The images were processed, reconstructed, and segmented in a semi-automated manner. A multistart registration of the reconstructed spinal surface with preoperative CT was performed.”
“Target registration error (TRE) in the region of the laminae and facets was then determined, using bone screw fiducials not included in the original registration process. each spine also underwent multilevel laminectomy, and TRE was then recalculated for varying amounts of gone removal.”
Dr. Paulsen told OTW, “We demonstrated the feasibility of using iSV to capture 3D surfaces of the spine intraoperatively and co-registering this information with the pre-procedure CT imaging for surgical navigations. Registration errors were small and comparable to those in standard image-guidance. The iSV approach is much faster and more convenient than image-guidance methods currently used in spine surgery, and hopefully would become more adopted as a result.”
“Image-based co-registration of spine data collected intraoperatively with iSV is not only possible but a practical option.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.