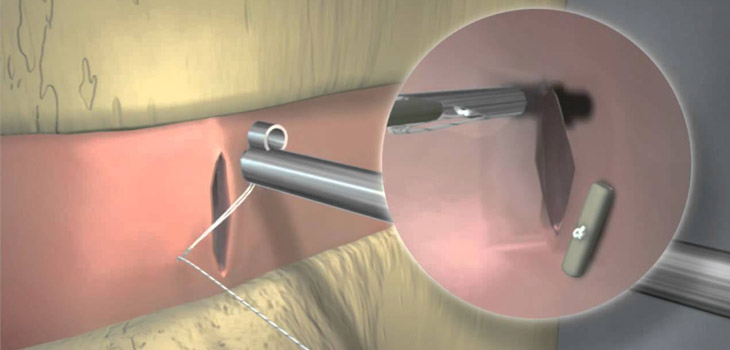
Annular repair. Fixing the rent in the annulus that can often occur because of minimally invasive spine surgery. Fixing the tear will lower re-herniation rates—at least that was the experience that Anulex Technologies, Inc. documented with its thousands of patients treated.
Anulex Died, But There’s More to the Story
7 min read Premium comments
#fda#annularrepair#anulextechnologies
Fixing the annulus is hard to do. The process is not intuitive. Anulex invented a solution. That solution, named Xclose, was employed thousands of times to close the annulus following discectomy surgery before the company went out of business in 2014.
What happened?
The FDA happened—but in an unexpected way.
And…that’s not the end of the story.
Annular Repair
OTW talked with two veterans of the Anulex experience—John E. Sherman, M.D., a spine surgeon with Twin Cities Orthopedics and a former consultant for Anulex and Scott L. Blumenthal, M.D., an orthopedic surgeon with the Texas Back Institute and a former consultant for Anulex.
“Annular repair,” Sherman said, “is necessary because microdiscectomy frequently fails. The rate varies but around 15% of the time you are going to have a symptomatic disc reherniation.”
Is there any other orthopedic procedure with a 15% reoperation rate? Total hips? Total knees?
Of course not. As Sherman told OTW: “If you had total hips or total knees that 15% of the time you had to take them back and revise them, people wouldn’t be happy with that.”
The most common reason, said Sherman, for microdiscectomy failure is a persistent defect in the annulus. But fixing the defect is hard to do. Because of the spinal anatomy, annulus is hard to suture. So, there was a clear need for a device which would simply and safely close the annulus and, thereby, cut that 15% risk of re-surgery for herniation down to practically zero.
Anulex’s System
Minnesota-based Anulex Technologies, Inc. was founded in 2001 and came out of an incubator that was formed by Dale Spencer who was the CEO of SciMed. Spencer had helped found more than a dozen medical device companies. Spencer was on the corporate board of Anulex for its whole existence.
Sherman said, “He took engineers from SciMed and said you are going to be the team that runs Anulex. The original engineer who ran Anulex was Matt Burns.”
Sherman was first introduced to the company by Burns. He asked Sherman to do their initial cadaver lab for the Xclose System, and although there were a few kinks in that first initial concept, after more research and development they zeroed in on what they believed to be a safe and effective way to fix a tear in the annulus.
Is the Annulus a Soft Tissue? (Not a Trick Question, Honestly)
Together Sherman and Blumenthal described what happened beginning in 2006, which started off well.
That was the year that Anulex received 510(k) clearance from the FDA to market the Xclose Tissue Repair System as a Class II device since it was like existing Anulex anchor band suturing systems.
The language of the clearance, however, turned out to have an unexpected trap.
The FDA cleared Xclose for “use in soft tissue approximation for procedures such as general and orthopedic surgery”.
Soft tissue. Like an annulus, right? Not bone, for example.
So, Anulex began to market Xclose to spine surgeons to use on the annulus soft tissue to fix tears resulting from discectomy procedures.
Remembers Blumenthal, “Anulex approached a number of sites around the U.S. with this technology with the labeling of soft tissue repair. I thought the technique was very amenable, very easy to take care of a problem that is otherwise technically almost impossible to take care of.”
In addition, Anulex began a prospective, randomized study of annular repair with Xclose in 2007, and posted the study on clinicaltrials.gov—as is required for any study which would like to be published in a peer review journal.
The study investigators enrolled 750 patients. They randomized patients to annular repair and to no repair following a microdiscectomy. All patients were expected to complete their two-year follow-up in October 2011.
In February 2010, Anulex began marketing the Xclose Tissue Repair System.
The FDA Comes Calling
On learning about the study and the commercial release of the device the FDA’s Minneapolis District Office inspected Anulex’s facilities in Minnetonka, Minnesota, in August and September 2010.
That inspection led to a February 2011 warning letter stating that Anulex had mislabeled the Xclose device and needed an FDA approved Investigational Device Exemption (IDE) to test the device on patients.
According to the FDA, annulus repair is not soft tissue repair.
John Sherman, who is a calm Midwestern surgeon, simply said that the FDA’s conclusion was nonsensical.
But the FDA’s charge was serious because it effectively accused the company of putting patients at risk by enrolling them in an unauthorized clinical trial.
Anulex had no choice but to shut down the study.
Are 34 Institutional Review Boards Wrong?
Thirty-four Institutional Review Boards (IRBs) reviewed the study, the company and the device and approved using Xclose on patients for this study. Furthermore, said Anulex, medical device regulatory experts, health professionals and surgeons all looked at the Xclose and no one said that an IDE was needed.
On top of that, there had been no unusual patient safety issues or adverse events.
As the company told OTW at the time: “Anulex is steadfast in its commitment to conducting its business in full compliance with all regulatory and statutory requirements. While we respect the FDA’s perspective in this matter, we are disappointed to have received the FDA’s letter because we firmly believe our post-market activities related to Xclose have complied with FDA law.”
Sherman, who was also a member of Anulex’s board of directors, remembered, “At the board level we seriously considered suing the FDA because of the capricious decision that the annulus was not soft tissue, that it was something completely different from other predicate devices that we had.”
The board did not ultimately sue the FDA.
Anulex complied with everything the regulators asked.
All marketing for Xclose was changed to clearly be for general and orthopedic surgery only. Management shut down the study. They also met with the FDA several times in the hopes of receiving approval for the device to be used during discectomies to repair the annulus.
For Sherman, the most disturbing part of these multiple meetings with the FDA was hearing the FDA reviewer make a scientifically inaccurate comment that the closing the annulus could cause paralysis in patients if somehow the Xclose device entered the spinal canal.
To understand how improbable that concern was, Dr. Sherman pointed out that the device was only 1mm by 3mm and said, “You can put in 30 of them in and if they came out, the patient would still not be paralyzed.”
Arguing Spinal Anatomy With the Reviewer
Sherman still remembers arguing spinal anatomy with the reviewer.
The reviewer didn’t change her opinion. All the way through the process there was this recurrent theme of catastrophic neurological deficit if the device displaces, even though there was no scientific basis for it.
Blumenthal added that there were thousands of patients who had an Xclose implanted, those done in the study setting and those performed outside of the study, and as far as they know no one had become paralyzed because of the device.
Unfortunately, when the meetings with the FDA ended up going nowhere and their financing dried up, the company shut down in 2014.
Now, the Rest of the Story
If John Sherman and Scott Blumenthal thought that this was the end of their annular repair journey—they were about to be find out differently in Berlin.
At a spine meeting in Berlin, Germany, in October 2017, John Sherman was cruising the exhibit hall when he noticed a table with devices that looked suspiciously like annular repair instruments.
Sherman asked a company representative standing at the table if the FDA had cleared these devices. The answer was…wait for it…”YES.”
“Of course, you could have pushed me over with a feather,” Sherman told OTW.
The company Sherman was talking to was a Canadian firm named Anchor Orthopedics XT, Inc., located in Mississauga, Canada.
As Blumenthal explains, “Anchor is permitted to market these closure devices for disc repair, but not for annular repair. It was a fascinating kind of thing and I had the same reaction as John did. What do you mean you were approved for this?”
Disc Repair
Both Sherman and Blumenthal ended up meeting with representatives from the company at their headquarters to learn more about their product.
“The best I could gather from when we met with them, they just had better FDA consultants and a better law firm to get the labeling in the U.S.,” Blumenthal said.
On the future of annular repair, Blumenthal said that while Anulex’s Xclose system worked and was easy to use, surgeons are not going to want to revisit a medical device that has already come and gone.
Anchor is new to the U.S. and is just now getting its marketing and sales effort launched. As Blumenthal explained to OTW, Anchor is developing a marketing and sales team in the U.S. that can reach the people who are doing the microdiscectomies. “When I first met Anchor Orthopedics, they had their own sales team but none of them knew the surgeons in the market, so they had to make cold calls. So, they are starting to develop connections with distributors that have relationships with spine surgeons.”
And, a lot has changed since Xclose received its 510(k) in 2006. The rise of the Ambulatory Surgery Center (ASC) has changed the minimally invasive surgery (MIS) and microdiscectomy market which, in turn, will influence Anchor’s disc repair product—particularly with regards to reimbursement.
Reimbursement.
Like the FDA in a fun house.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.