Mayo Clinic’s Mark Pagnano, M.D. and his research team collected, analyzed and, now, reported the results of 10-year follow up on patients diagnosed with primary osteonecrosis and were treated with unicompartmental knee arthroplasty (UKA).
10-Year Uni Arthroplasty for Osteonecrosis Data
1 min read Premium comments
#kneereplacementSecondary#knee#osteonecrosis
The study was presented in the April 9, 2018 edition of The Bone and Joint Journal in a paper titled; “Reliable outcomes and survivorship of unicompartmental knee arthroplasty for isolated compartment osteonecrosis.”
The authors wrote, “A total of 45 patients underwent 46 UKAs for knee osteonecrosis between 2002 and 2014 at our institution…. Twenty patients (44%) were female; the mean age of the patients was 66 years, and mean body mass index (BMI) was 31 kg/m2. Of the 46 UKAs, 44 (96%) were medial UKAs, and 35 (76%) were fixed-bearing design. Mean mechanical axis postoperatively was 1.5° varus (0° to 5° varus); 41 UKAs (89%) were performed for primary osteonecrosis….”
Mark Pagnano, assistant professor of orthopaedic surgery at Mayo Clinic in Rochester, Minnesota, and co-author on the study told OTW, “Because osteonecrosis often involves only one portion of the knee joint it is logical to wonder whether partial knee replacement is a good treatment choice. We specifically wanted to know if the cause of osteonecrosis or the amount of dead bone would adversely impact the result. By including patients with osteonecrosis secondary to systemic steroid use we had additional patients with large areas of dead bone.”
“We found that unicompartmental knee replacement for primary osteonecrosis was reliable, reproducible and durable out to 10 years. Also, unicompartmental knee replacement for secondary osteonecrosis had a substantially higher risk of revision or reoperation.”
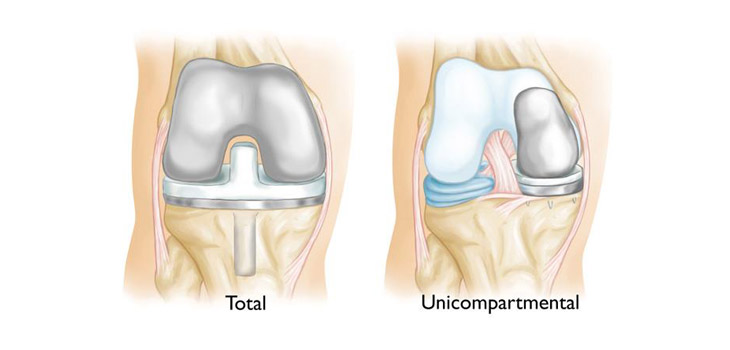
“While unicompartmental knee replacement is a smaller operation with a quicker recovery, it appears that for many patients with secondary osteonecrosis of the knee the higher risks of revision and reoperation with unicompartmental knee replacement may make total knee replacement a better choice.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.