Pediatric Osteoporosis Linked to Anti-Inflammatory Meds
Pediatric Osteoporosis Linked to Anti-Inflammatory Meds?; Tool Identifies Risk for Dislocations After THA; Do Higher Volume Hospitals=Better Value in Hip, Knee Revision?
6 min read Premium comments
#osteoporosis#hip#glucocorticoid
Adolescent mice—reportedly easier to work with that adolescent humans—are helping us understand how cells that age prematurely (senescent cells) may emanate from poor bone mass in youth…and how glucocorticoid given during puberty for inflammation resulting from rheumatoid disorders and other diseases might be the origin of that premature aging.
The article, “Programmed cell senescence in skeleton during late puberty,” was published in the November 3, 2017 edition of Nature Communications.
Mei Wan, Ph.D., a professor of Orthopaedics at Johns Hopkins University in Baltimore, and co-author on the study, told OTW, “Childhood and adolescence are critical periods for optimizing bone growth and mineral accrual. Bone mass and strength in this period are influenced by genetic/epigenetic factors, activity, nutrition, and hormones. For children with genetic skeletal disorders or chronic disease, bone growth and mineral accrual are often compromised, leading to osteoporosis and high bone fracture rate.”
“In childhood, fractures are a common event, with an annual fracture incidence of 205 per 10,000 person-years in those under the age of 16 years, with the highest rate during the rapid growth spurts of puberty.”
“Moreover, bone mineral accrual in childhood and adolescence influences long-term bone health. Epidemiologic studies suggest that 60% of the risk for osteoporosis later in life can be explained by the bone mineral acquired by childhood and early adulthood. However, little is known about the cellular changes and the regulatory mechanisms in the skeleton during the transition from fast growing childhood/early puberty to slow growing late puberty/young adulthood.”
“Childhood osteoporosis is typically divided into primary and secondary causes, with osteogenesis imperfecta (OI) representing the prototypical primary osteoporosis of childhood.”
“There is a growing list of secondary pediatric osteoporosis (i.e., osteoporosis caused by underlying diseases and/or their treatment), with most falling into two broad categories: glucocorticoid-treated diseases and the disorders which compromise normal weight-bearing and mobility such as cerebral palsy, Rett syndrome, Duchenne muscular dystrophy, spina bifida, and spinal muscular atrophy.”
“Glucocorticoid-induced osteoporosis is the most common form of secondary osteoporosis. Long-term treatment of glucocorticoids has been widely used in the management of chronic inflammatory childhood illnesses such as rheumatoid disorders, Crohn’s disease, nephrotic syndrome as well as rare genetic diseases such as Duchenne muscular dystrophy.”
“Although the use of glucocorticoid has led to improved outcomes and survival rates, it is at the cost of substantial adverse effects on bone. Epidemiologic studies have shown an up to 34% prevalence of vertebral fractures in children and youth with long-term glucocorticoid therapy.”
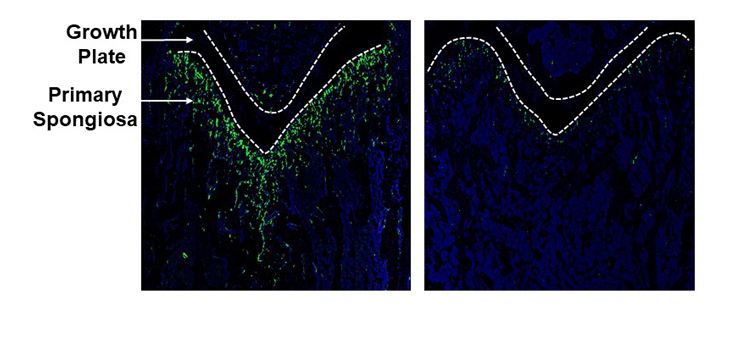
“This study aims to understand how epigenetic mechanisms control bone growth/accrual during childhood and adolescence. We found that mesenchymal stem/progenitor cells (MSPCs) in primary spongiosa of long bone during late puberty undergo a normal programed senescence, which is epigenetically controlled by a polycomb histone methyltransferase Ezh2 and its H3K27me3 mark. Premature acquired senescence during early puberty leads to impaired angiogenesis and osteoblastogenesis as well as bone loss in later adult life.”
“Glucocorticoid treatment also caused early onset cellular senescence in primary spongiosa of long bone during early pubertal mice.”
“Importantly, GSK-J4, a specific H3K27 demethylase inhibitor, elevated H3K27 methylation, blocked the early onset cellular senescence, and rescued the bone-loss phenotype induced by glucocorticoid treatment. Our finding establishes MSPC senescence as a normal programmed cell fate change in postnatal skeleton and demonstrate proof-of-concept for targeting Ezh2-H3K27me3 in juvenile osteoporosis.”
Tool Identifies Risk for Dislocations After THA
Jonathan Vigdorchik, M.D., assistant professor of orthopedic surgery and associate fellowship director of the Division of Adult Reconstructive Surgery at NYU Langone Health, and his colleagues set out to learn more about who exactly is at risk for postop total hip arthroplasty (THA) dislocations…and what can be done about it.
Dr. Vigdorchik, study co-author, told OTW, “In the past, surgeons minimally thought about who was at risk for a complication prior to surgery.”
“Hip replacement is a great procedure with a low complication rate, so it was not really necessary to think about. However, recently with the increasing quality of care from bundled payment initiatives, surgeons are paying attention to things that can help decrease risk of complications such as infection and readmission.”
“A big part of this is dislocation in THA, as it is the most common cause of revision THA. Therefore, we sought out to determine which patients are at higher risk of dislocation and what can we do to prevent this from happening.”
“Beginning in 2016, surgeons used the standardized risk prediction model and treatment algorithm developed at NYU Langone, which factored in data collected from preoperative imaging taken while the patient was sitting and standing, and other measures that might affect risk for dislocation, including presence of degenerative spinal pathology, spinal deformity, or a prior lumbar fusion. Using the risk assessment tool, the researchers identified 192 of 1,009 patients as high risk for a dislocation after surgery.”
“All 192 patients underwent a total hip replacement through the high-risk algorithm, with dual mobility implants being used in 143 of the cases.”
“We found that patients with a spinal fusion of greater than three levels were patients that were the highest risk. There are also cumulative risks, such as a spinal fusion of one or two levels combined with a stiff spine. These high-risk patients need specific targets for their hip replacement, found out through a far more detailed preop workup than previously performed. Some of them also need use of computer navigation or even a dual mobility prosthesis to help mitigate the risk.”
“The biggest recommendation is really a thorough preop workup including a standing and sitting X-ray of the pelvis and also the lumbar spine. This will help to determine through the algorithm which patients are at risk.”
The study has been submitted for publication.
Do Higher Volume Hospitals=Better Value in Hip, Knee Revision?
Research recently presented at the annual meeting of the American Academy of Orthopaedic Surgeons (AAOS) found that low volume hospitals had a higher mean hospital-specific charge when it comes to hip and knee revisions.
The study, “Do higher-volume hospitals provide better value in revision hip and knee arthroplasty?” appears in the December 2017 edition of The Bone & Joint Journal.
Nicholas B. Frisch, M.D., M.B.A. is a hip and knee replacement surgeon at the DeClaire LaMacchia Orthopaedic Institute in Rochester, Michigan, and was a co-author on the study. Dr. Frisch told OTW, “There have been others who have reported on concept of volume and quality. Both hospital and surgeon volume have been studied. Higher volume hospitals have been associated with lower risk of complications following TKA and THA [total hip arthroplasty]. Few studies have reported on whether higher volume also correlates with lower cost of care.”
“We used the CMS (Centers for Medicare and Medicaid Services) Hospital Compare Database which includes data on 4,788 hospitals. We also accessed the Medicare Provider Utilization and Payment Data Inpatient Charge Data for 2014. We excluded hospitals with <11 DRG [Diagnosis-Related Group] episodes during the year studied. We identified all hospitals with data from patients in DRG 470. Ultimately, we identified 2,702 hospitals, [that] performed a total of 458,259 primary arthroplasty procedures in 2014. Low performing defined as <100 procedures per year. We collected patient satisfaction scores and 30-day readmission and risk-adjusted complications.”
Craig Della Valle, M.D. is chief of Adult Reconstructive Surgery and Professor of Orthopaedic Surgery at Rush University Medical Center. Dr. Della Valle, also a co-author on the study, told OTW, “In our study, 47% of hospitals were classified as low volume; low volume hospitals performed only 12% of primary joint arthroplasty cases. We also found that low volume hospitals had a higher mean hospital-specific charge and were more likely to be in a non-urban area. High volume hospitals had a higher star rating and performed better on every HCAHPS [Hospital Consumer Assessment of Healthcare Providers and Systems] metric.”
Dr. Frisch added, “Low volume facilities could potentially benefit from adopting some of the practices in place from high volume centers.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.