Researchers are beginning to shake things up with respect to hip arthroscopy for dysplasia.
Hip Dysplasia: High Incidence, Surprising Findings
2 min read Premium comments
#hipreplacementSecondary#arthritis#hipdysplasia#hip
New multicenter research indicates that, among other things, borderline to mild hip dysplasia without the presence of significant arthritis may be a reasonable indication for hip arthroscopy. Dean K. Matsuda, M.D. is with the DISC Spine and Sports Center in Marina del Rey, California. Dr. Matsuda is a co-author on a new study entitled, “Hip Dysplasia: Prevalence, Associated Findings, and Procedures From Large Multicenter Arthroscopy Study Group.” The research appears in the February 2018 edition of Arthroscopy.
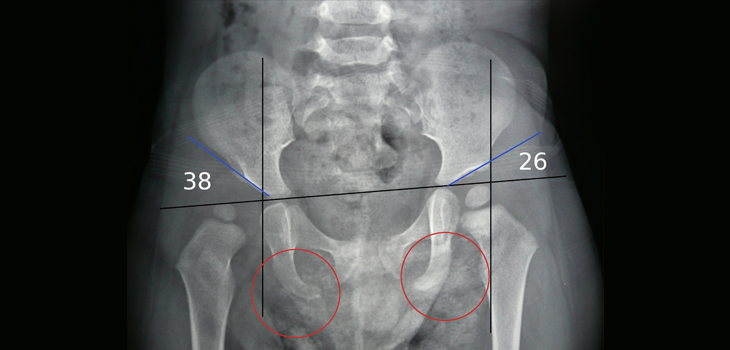
Dr. Matsuda told OTW, “Hip dysplasia is a common cause of pain, chondrolabral pathology, and secondary arthritis often leading to hip replacement surgery in relatively young patients.”
“Although I admit that I was one of the surgeon-investigators to publish caution when using hip arthroscopy in this setting that study involved few patients with marked dysplasia in an era preceding capsular closure, despite having labral repairs and femoroplasties for associated cam femoroacetabular impingement (FAI). The key findings of our recently-published observational study done by the MASH study group with >1000 patients is that a relatively high prevalence of patients (13%) that underwent primary hip arthroscopy by seven high-volume experienced U.S. surgeons had borderline to mild dysplasia and 80% of those patients had a cam deformity.”
“The study showed that dysplasia patients without cam morphology had increased flexed-hip internal rotation (FIR) on anterior impingement examination compared to normal controls, whereas those with associated cam morphology had significantly decreased FIR.”
“Takeaway practical points from this study are that:
- borderline to mild hip dysplasia is considered a reasonable indication for hip arthroscopic treatment by this set of surgeons,
- cam morphology is commonly associated with dysplasia,
- patients with nonarthritic hip pain and increased or normal FIR on anterior impingement examination may still have chondrolabral pathology and may still be candidates for hip arthroscopy (some insurers require decreased FIR as a requirement of medical necessity for hip arthroscopy), and
- Decreased FIR in dysplasia should encourage the detection and eradication of co-existent cam FAI.”
“This observational study demonstrates what is being done, but not necessarily what should be done. In regards to borderline to mild dysplasia, emerging outcome studies are reporting arthroscopic outcomes approaching those successful outcomes for FAI and labral tears.”
“In contrast to my early study, it appears that minimal to mild dysplasia without significant arthritis may be an indication for hip arthroscopy when it includes a comprehensive treatment of chondrolabral pathology, cam decompression, and capsular closure (or possibly mini-capsulotomies). The MASH group will soon be reporting high volume multicenter arthroscopic outcomes of dysplasia compared with normal controls. Stay tuned as we believe this may change the way many view hip arthroscopy for dysplasia.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.