Each year, more than 300,000 Americans receive a hip replacement. Now doctors at The Ohio State University Wexner Medical Center are using a procedure called subchondroplasty to give patients with damaged hips treatment options other than a hip replacement.
Subchondroplasty Viable Option for Hip Joint Replacement
1 min read Premium comments
Secondary
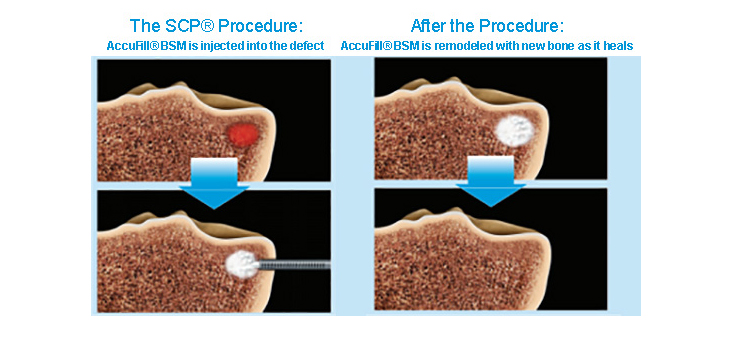
Subchondroplasty requires a doctor to bore a small hole in the hip joint and use it to inject a bone substitute material into the joint filling any voids and open spaces. Over time the patient’s body replaces the bone-substitute material with their own healthy bone.
The procedure was first popularized for knee patients and has developed a strong record of successful outcomes. Increasingly, it is also becoming a viable option for patients who would otherwise be candidates for a hip joint replacement surgery.
“We want to preserve the native hip whenever possible because once you have a hip replacement, there’s no going back,” said Dr. Kelton Vasileff, an orthopedic surgeon at Ohio State Wexner Medical Center, who told a writer for Medical News, “We’re able to use a bone-hardening procedure that’s traditionally been used in knee surgery to help repair a patient’s own hip joint.”
Vasileff, who specializes in hip preservation surgery, said that in the past, a replacement would be the only long-term option for a lot of patients. He believes that this procedure allows him to add support to the bone, making more damage-reversing surgeries possible.
Vasileff noted that there is a finite lifespan to some implants, as they are typically made from metal or ceramic on plastic articulations. “Problems with implants down the road could mean more surgery for these patients, and that’s always more difficult than doing it for the first time.”
Subchondroplasty is also much less invasive than a total hip replacement, which allows patients to get back on their feet sooner. Vasileff uses it in conjunction with other treatments to help patients preserve the hip joints they were born with for as long as possible.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.