When an athlete is injured, the big question is always, “Is surgery the best treatment option for me and will it reduce the risk of re-injury?” In a study, “Treatment of Primary Acute Patellar Dislocation: Systematic Review and Quantitative Synthesis of the Literature,” published in the November 2017 issue of the Clinical Journal of Sports Medicine, researchers tried to answer that question and found that while surgical treatment of primary acute patellar dislocation had better short-medium clinical outcomes than a more conservative approach did, long-term results were similar for both types of treatment.
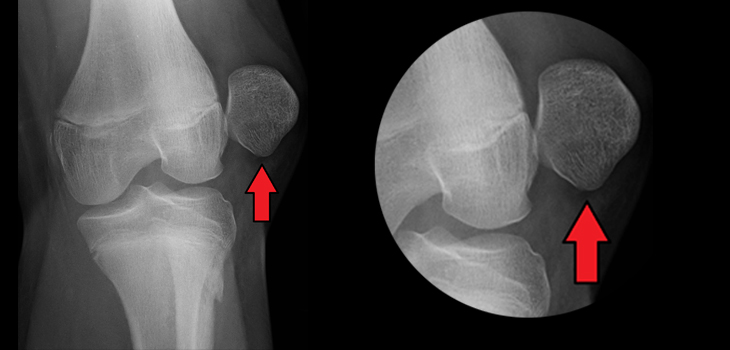
Patellar Dislocation: Does Surgery Give Best Results?
1 min read Premium comments
Secondary
The researchers did a comprehensive search of PubMed, Medline, CINANL, Cochrane, Embase, and Google Scholar databases for studies on primary acute patellar dislocation and collected data on 2,086 patients and a total of 2,134 knees. The average age of patients at dislocation was 20.3 years.
According to the data, the average Kujula score was 75.6 for patients treated conservatively and 88.7 for patients undergoing surgical treatment in the short-medium follow-up (less than five years). When it came to long-term follow-up (more than five years), patients treated conservatively had an average Kujula score of 87.5 and patients undergoing surgical treatment had a score of 86.6.
The rate of recurrence was lower in the surgical group (25%) than in the conservative group (36.4%). The complication rate for the surgical group was 6.5%. There were no complications in the conservatively treated group.
Because both groups had good long-term follow-up results, the researchers called for further randomized controlled trials to study the anatomical abnormalities and soft-tissue integrity that may influence the choice of treatment.
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.