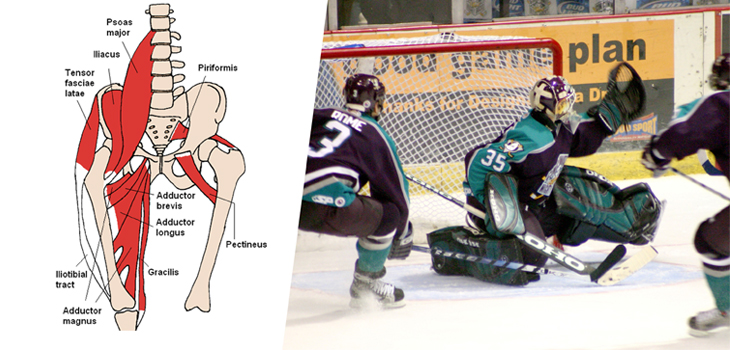
In a new study, “Epidemiology of Hip Flexor and Hip Adductor Strains in National Collegiate Athletics Association Athletes, 2009/2010-2014/2015,” published in the October, 2017 issue of The American Journal of Sports Medicine, researchers discovered that the male National Collegiate Athletics Association athletes, most specifically men’s soccer and men’s ice hockey players, had the highest rates of hip flexor and hip adductor strains.
Hip Adductor Strains a Real Pain for Male Athletes
1 min read Premium comments
Secondary
The researchers took a convenience sample of National Collegiate Athletics Association (NCAA) varsity teams from 25 sports and examined rates and distributions of strains by mechanisms, recurrence, and participation restriction time during the 2099/2010-2014/2015 academic years.
According to the data, there were 770 hip flexor and 621 hip adductor strains, with an overall injury rate of 1.60 and 1.29 per 10,000 athlete-exposures, respectively. The highest rates of strains were found in men’s soccer and men’s ice hockey, and most of them occurred during practice not game time.
In sex-comparable sports, the researchers did not see a difference between men and women when it came to rate of hip flexor strain rates, but did find that the rate of hip adductor strains was higher in men than women. Interestingly enough most of the strains were noncontact injuries (hip flexor strains, 59.4%; hip adductor strains, 62.5%). The highest rates of recurrence of both types of strain were found in men’s and women’s ice hockey.
The researchers wrote, “Male sports teams, especially soccer and ice hockey, should place an emphasis on prevention programs for hip adductor strains. Secondary prevention programs involving thorough rehabilitation and strict return-to play criteria should be developed and implemented to curb the high recurrence rate of these injuries, particularly in ice hockey.”
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.