Medical history is made when brave surgeons encounter equally brave patients. The patient in his case is 20-year-old Penelope Heller. Leading the surgery on Heller was Jeffrey L. Port, M.D, attending cardiothoracic surgeon at New York Presbyterian /Weill Cornell Medical Center.
3D Printed Sternum/Ribcage Implanted in Surgical First
2 min read Premium comments
Secondary
Port undertook the operation to revise a prior sternum/ribcage removal and reconstruction done in 2014. The patient had undergone the original procedure to remove a malignant bone tumor that was resistant to chemotherapy.
Doctors successfully removed the cancer in the first surgery and installed an off-the-shelf implant for the patient. However Heller continued to experience pain and difficulty breathing.
As she explained, “With a long active life ahead of me I wanted to participate in activities that I love fully and without pain. Electing to have this procedure was a big decision and I’m coming forward to empower other people in the same situation.”
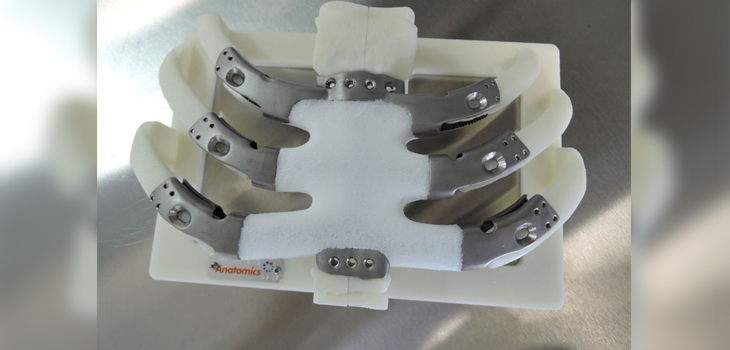
The surgery, performed on August 2, 2017, replaced the sternum and partial ribcage using a custom 3D printed composite titanium/porous polyethylene implant.
It was the first time that this technology was used in the United States and only the second time in the world that a 3D printed composite sternum and rib cage had been implanted. The implant was used under the FDA’s Expanded Access (Compassionate Use) Program.
Researchers designed the implant using high resolution CT scans of the patient’s chest that were sent to Anatomics Pty Ltd engineers. Port reviewed and confirmed the design before it was sent to Australia’s Commonwealth Scientific and Industrial Research Organization’s printing laboratory.
Heller’s custom sternum implant became the second in the world to also use Australia’s Porestar technology, a proprietary porous polyethylene material with bone-like architecture.
Porestar is currently awaiting FDA marketing approval.
Anatomics executive chairman Paul D’Urso, said, “The patient’s story is one of many but what makes it truly remarkable is how the patient and her family, Dr. Port and the staff at New York Presbyterian/Weill Cornell, Anatomics and the FDA came together to make this story a reality. It was a group effort that began with the patients pursuit of information.”
A media source in New York reports that the patient is doing well.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.