Histogenics Corporation, a regenerative medicine company headquartered in Waltham, Massachusetts, recently announced the completion of patient enrollment for Phase 3 Clinical Trial for NeoCart in accordance with the Special Protocol Assessment (SPA) agreement with the FDA.
Histogenics Moves onto Phase 3 Clinical Trial for NeoCart
1 min read Premium comments
Secondary
According to a recent press release, “NeoCart is a tissue-engineered cartilage implant created from a patient’s own cells. The patient’s cells are multiplied in Histogenics’ laboratory and then infused into a proprietary scaffold to allow them to function like native cartilage.”
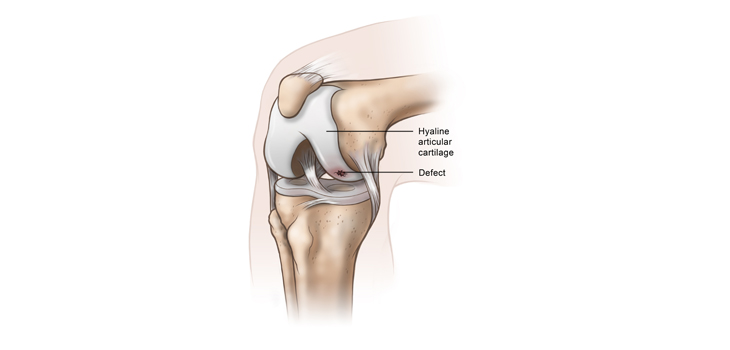
Data so far suggests that it can potentially accelerate recovery and reduce pain compared with microfracture, the most common treatment for knee cartilage defects. During microfracture, small holes are made in the bone to heal the cartilage.
The randomized Phase 3 clinical trial will evaluate the safety and efficacy of NeoCart compared to microfracture in 245 patients at over 35 sites in the U.S. and Canada.
The primary endpoint is a dual-threshold responder analysis measuring the improvement in the pain and function of each patient treated with NeoCart compared to those treated with microfracture one year after treatment.
Adam Gridley, president and CEO of Histogenics, told OTW in an interview, “We think it is a very unique endpoint and a pretty high bar to achieve.”
“What makes NeoCart unique is that we are creating full functioning new tissue outside the body. Based on early results, NeoCart provides earlier pain relief and safe and durable results. Patients will be back to function quicker than they would with microfracture.”
He added, “With microfracture there is a lot of variation in response. There is a 30% reoperation rate after 2-3 years and oftentimes osteoarthritis will develop.”
Gridley said that they are on track for top-line year superiority data and potential BLA (Biologics License Application) Filing in third quarter of 2018.
Author
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.