Pinnacle Spine Group, LLC, based in Dallas, Texas, has been granted a U.S. Patent No. 9,649,203 titled “Methods of Post-Filling an Intervertebral Implant” that reinforces the company’s exclusivity position with respect to its in situ graft delivery technology.
Pinnacle Awarded Patent for Better Void Fill
1 min read Premium comments
Secondary
Like previously issued patents, it relates to the delivery of graft material to fill the internal chambers of a spinal fusion device, while allowing for graft material to be in contact with the endplate surfaces of the adjacent vertebral bodies.
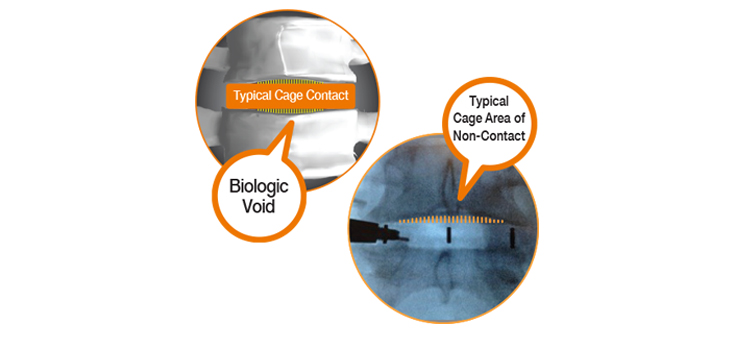
Pinnacle Spine Group has built a platform technology around the novel concept of delivering bone graft material in situ, into the implanted device and to fill any remaining biologic void NOT covered by other spinal fusion systems, according to company President Zach Sowell.
“Years ago, we identified a problem with traditional interbody fusion systems—that a biologic void remained between an implant and its two adjacent vertebrae,” said Sowell.
“We developed a highly effective solution and are thrilled to now have even stronger patent protection related to in situ graft delivery directly to an implant, a technique whose value is being recognized and appreciated by the spinal fusion industry.”
“This recognition is a testament to the technology’s usefulness and benefits, and we look forward to working with companies that are interested in adopting and using implant designs that require delivery of bone graft material in situ.”
Sowell said that Pinnacle Spine’s InFill Fusion Systems include an array of innovative fusion devices engineered for easier insertion, reduced subsidence through maximum contact with the apophyseal ring, a generous bone grafting area, and compatibility with the InFill graft delivery system.
The backbone of the technology is predicated on controlled and precise in situ placement of bone graft material directly into the implanted device, to achieve maximum contact with the adjacent vertebral endplates.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.