The FDA has granted expanded 510(k) clearance for Minnesota-based Spineology, Inc.’s Elite expandable interbody fusion system. The company completed a limited release of the system in November 2016.
Spineology Expandable Interbody Fusion System Cleared for Allografts
1 min read Premium comments
Secondary
This clearance adds a narrower, 10mm, version of the device and an indication to utilize the devices with allograft bone.
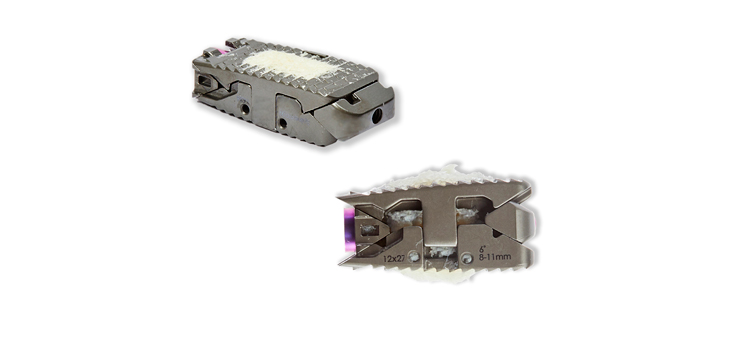
The implant is inserted into the disc space and is expanded once in position to restore anatomic disc height, provide column support, and facilitate indirect decompression. It is designed with titanium alloy and has a large graft window to enable bone through-growth and maximize fusion.
John Booth, the company’s CEO, stated in a March 13, 2017 press release, that the broader size offering and the allograft bone indication, “allow the surgeon to pair Elite with Incite Cortical Fibers. Incite’s excellent handling properties and ability to expand in-situ with the Elite Implant are added benefits not found in competitive systems.”
Incite Cortical Fibers, according to the company, are fiber-based bone allografts that are naturally osteoconductive and that are carefully processed to maintain their inherent osteoinductive potential. These freeze-dried grafts expand when hydrated in-situ, eliminating concern of graft off-loading following implant expansion.
Mark Grubb, M.D., of the Northeast Ohio Spine Center, said, “The minimal initial starting height and a 10mm wide footprint reduces neural retraction requirements. Additionally, having the Incite bone graft that expands with the implant helps ensure good graft apposition.”
The company says Dwight Tyndall, M.D., with the Orthopaedic Specialists Northwest Indiana, uses Elite with the Spineology ACT MediaLIF posterior mid-line approach. “The multiple width, length, and lordosis options make Elite an excellent choice for the mid-line approach and bilateral implant placement,” said Tyndall.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.