Ah, the pain that travels…so fun. There are loads of patients who live with low back pain that radiates to the buttock, groin, thigh, and even knees. But where does the pain start? A new article published in the February Journal of the American Academy of Orthopaedic Surgeons (JAAOS) describes the identical symptoms associated with hip and spine pain and discusses the diagnostic steps and tests required to treat them appropriately. The article is entitled, “Differentiating Hip Pathology From Lumbar Spine Pathology: Key Points of Evaluation and Management.”
Where Does That Back Pain Really Come From?
2 min read Premium comments
Secondary
“In these instances, similar or overlapping symptoms may delay a correct diagnosis and appropriate treatment,” said article author Afshin Razi, M.D., an orthopedic surgeon and clinical assistant professor at New York University Langone Hospital for Joint Diseases, in the February 6, 2017 news release.
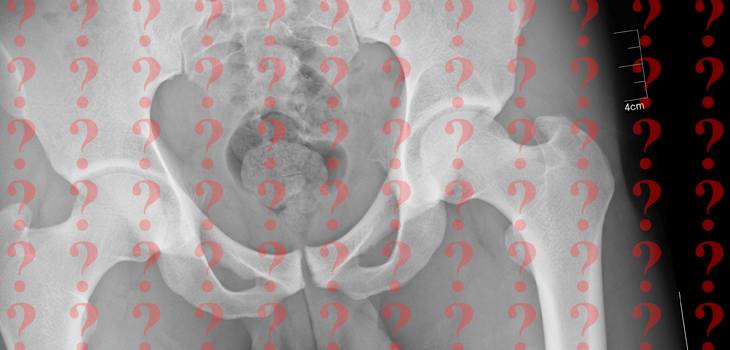
“Plain and advanced imaging studies and diagnostic injections also can be used to further delineate the primary problem and guide the appropriate sequence of treatment,” said Dr. Razi.
“Focusing on both the spine and the hip as potential causes of pain and disability may reduce the likelihood of misdiagnosis, and the management of conditions affecting the spine and/or hip may help reduce the likelihood of persistent symptoms,” said Dr. Razi.
Dr. Razi told OTW, “As an orthopaedic surgeon specializing in spine surgery I encounter many patients who present with concomitant back and hip pain. Many of these patients are also referred to me by surgeons who solely take care of hip problems such as total hip replacement or sport medicine specialist who treat younger patients with hip pain. It can be very difficult to properly diagnose the main issue and as such some patients go on to have unnecessary treatments, including surgery, because of their persistent symptoms.”
“It was our goal to try to educate physicians, including orthopaedic surgeons, on the common differential diagnoses, appropriate clinical history and physical examination, diagnostic tools and their evaluations appropriately, as well as treatment options and priorities of which one to be treated first. More recently, it has been noted that some patients who have undergone total hip replacement with significant curvature of the spine had postoperative dislocation of the hip after reconstruction of the spinal malalignment. This article also talks about this newly seen problem.”
“We did an extensive literature search and through our two previous seminars on this topic we were able to gather information to aid our colleagues on best ways of differentiating causes of hip and back pain.”
“There is a major need for obtaining a thorough clinical history, performing a complete physical examination, and ordering with analyzing appropriate diagnostic tests followed by diagnostic and therapeutic injections can differentiate between hip problems versus back related pathologies. There also should be patient education with regard to complex hip-spine problems to make sure they’re aware that despite addressing one problem the other problem may also need to be addressed at some point.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.