It was time to reflect on the literature, say the authors of a new review article on osteogenesis imperfecta (OI). Researchers from the Department of Orthopedics at the Nemours/Alfred I. duPont Hospital for Children in Delaware delved into the latest on OI, a genetic condition typically involving bone fragility, multiple fractures, short stature, and scoliosis.
Osteogenesis Imperfecta: What’s Happening in the Spine?
2 min read Premium comments
Secondary
Suken A. Shah, M.D. is division chief of the Spine and Scoliosis Center at Nemours. He told OTW, “We felt that a thorough review and description of the problems and disorders of the spine in children with osteogenesis imperfect was necessary at this time. Not many new updates in orthopaedics were written in 15-20 years despite all of the new information in bone health, genetics and surgical techniques. Many families came to our center seeking treatment for spinal conditions due to OI after doctors in their area advised them that their conditions were too complicated or risky.”
“Kids with OI should be monitored for scoliosis; it can progress during the growth spurt and become quite severe very quickly, affecting their pulmonary function and quality of life. Traditional fusion techniques were fraught with complications, so my colleagues and I developed a multimodality protocol to treat these kids successfully.”
When it comes to lumbosacral pathology in these patients, Dr. Shah noted, “This is a rare disorder and regular X-rays do not illustrate the bone pathology very well. Doctors need to be better equipped with information and ‘what to watch out for.’”
“Bisphosphonates are usually effective in decreasing fracture frequency and improving bone density. Evidence exists that bisphosphonate therapy may decrease the risk of scoliosis progression. Patients with severe OI should be screened for spinal deformity and problems at the craniocervical junction, like basilar invagination. New techniques in pedicle screw instrumentation and screw augmentation can be used to treat severe scoliosis in these patients to improve pain, pulmonary function and quality of life.”
“Stiff curves in patients with bad bone need to be approached carefully. Airway management and positioning are important; the curve needs to be made more flexible, usually with rib releases and osteotomies. Matching the implant with the child’s bone is the key to success: multiple fixation sites with pedicle screws, sometimes augmented with bone cement and secondary fixation, results in better correction, avoids implant failure and usually achieves stable fusion.”
“Further research to study patient-related outcomes after scoliosis surgery in this population needs to be performed. Indications and best practices for craniocervical surgery need to be described. Efforts to improve bone fixation, optimize pain management after spinal surgery and reduce complications are underway at our center as well.”
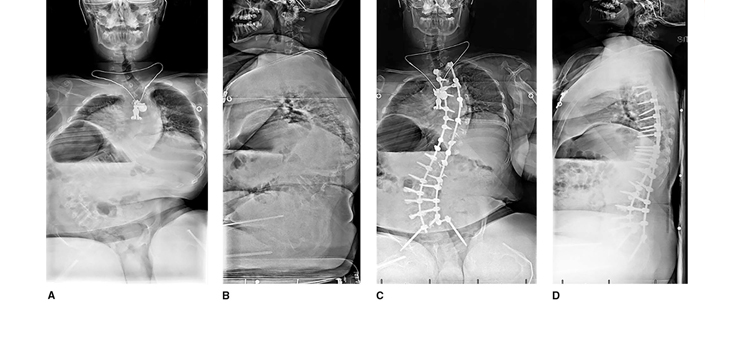
Image Caption: PA (A) and lateral (B) radiographs demonstrating severe osteogenesis imperfecta in a 16-year-old boy with an 87_ thoracic curve, a 115_ thoracolumbar curve, and substantial pelvic obliquity. PA (C) and lateral (D) radiographs obtained 2.5 years postoperatively demonstrate spinal fusion from T1 to the sacrum with cement-augmented pedicle screws and pelvic fixation.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.