For many years the standard in training airline pilots has been pre-flight simulators. This helps them become more skilled at flying the actual plane. This is a comfortable thought isn’t it? Exactly! Well, recent developments in shoulder replacement surgery allow surgeons to simulate surgery and this benefits not only the patient, but also the hospital. Jon J.P. Warner, M.D. is chief of the Massachusetts General Hospital Shoulder Service and co-Director of the Boston Shoulder Institute. He and his colleagues are bringing clarity to the operating room via patient-specific planning for shoulder replacement.
Patient-Specific Planning for Shoulder Replacement
2 min read Premium comments
Secondary
Dr. Warner told OTW, “Joint replacement is expensive and the results are unpredictable; and unlike total hip and knee surgery, most orthopedic surgeons have limited experience with shoulder replacement surgery. Since shoulder replacement surgery is performed at a volume of <15% hip or knee replacement surgery, 90% of all shoulder replacements in the U.S. are performed by surgeons who do less than 5 procedures each year. Thus these surgeons may not have enough experience to avoid some common problems. These problems may include incorrect size selection and inaccurate placement of the shoulder replacement components.”
“For shoulder replacement you must select a size that matches the patient’s anatomy, meaning that you have to have a full complement of instruments and implants on hand. To do a single operation the device manufacturer must deliver roughly $75, 000 in inventory of instruments and implants; and if the surgeon opens a tray and doesn’t use it then it’s $100 to sterilize it. This economic reality challenges both the hospital and the company to provide cost-effective care.”
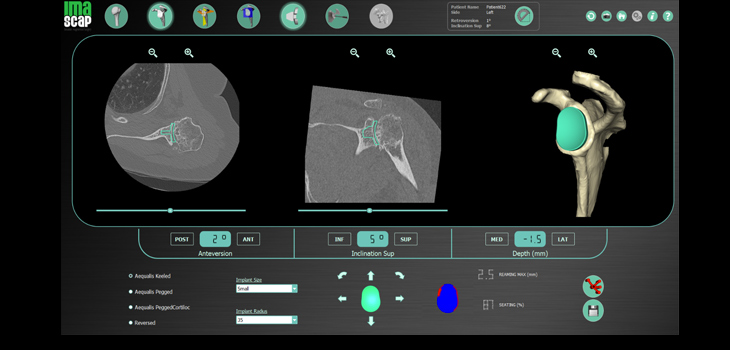
“A French company named IMASCAP has developed a software program (Glenosys) which is currently licensed to the Wright Medical Company as a program named BLUEPRINT. This program is available free of charge to surgeons who use this company’s implants. The software is unique since the surgeon simply uploads the CT scan Dicom images to a cloud software program that constructs a 3D plan of the shoulder and populates the desktop with the variety of implants and sizes for the shoulder replacement. The sequencing process takes only 90 seconds. The surgeon can then do the entire operation virtually and know the optimum placement and size of components—all of this happens on the surgeon’s laptop before going into the operating room (OR).”
“The beauty of this software is that it helps less experienced surgeons avoid errors. If the surgeon does something wrong the computer program warns the surgeon with a highlight of the error. For example, the glenoid component will turn red if it is placed so as to breach the glenoid vault and it turns green when it is properly positioned. Reaming and orientation can thus be easily controlled by the surgeon.”
“Patients feel reassured that their surgeon will avoid an error in component selection and placement. OR staff like it because it improves inventory management with very accurate size prediction prior to the actual surgery. Thus the surgery goes quicker because there is no guesswork in sizing and placement. The accuracy of socket determination and humeral head placement and sizing is about 95%.”
“And if you are not sure about something, you can plan the entire surgery out two different ways and have two options once you get into the OR. It is really an amazing tool.”
To view a video that provides insight into the program, visit www.bosshin.com/ and then go to “For Professionals” then to “Videos-Shoulder Arthroplasty.” View the video entitled “Virtual Shoulder Surgery”.
Dr. Warner indicates that he does have a conflict of interest.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.