Adolescent Obesity May Cause Permanent Bone Loss
Obesity and Permanent Bone Loss; Education Improves TKR for Patients; Avoid Tunnel Convergence in Knee Surgery
5 min read Premium comments
Obese teens could have permanent bone loss, says an ongoing study from Massachusetts General Hospital. The lead author, Miriam A. Bredella, M.D., is a radiologist at Mass General and associate professor of radiology at Harvard Medical School in Boston. She and her colleagues recruited 23 adolescents who were obese (mean age of 17 years and a mean body mass index (BMI) of 44 kg/m2) to participate in the study.
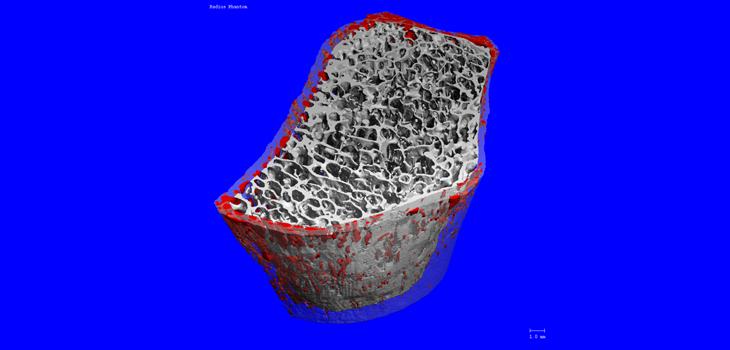
Dr. Bredella told OTW, “We used a computed tomography exam designed specifically for measuring bone mineral density and bone microarchitecture in the arms and legs; specifically, we measured the bone structure of the distal radius. We also used dual-energy x-ray absorptiometry (DXA) exams to determine body composition, including lean mass and visceral fat mass.”
The researchers found that BMI was positively associated with cortical thickness and area. Visceral fat mass was positively associated with cortical porosity. Lean mass was positively associated with trabecular density, volume and integrity. Given these findings, say the authors, it is possible that having significant visceral fat, as well as a low amount of muscle mass, can contribute to the risk for weakened bone structure in adolescents.
“Adolescence is a critical time for bone accrual, and peak bone mass (achieved by the mid-20s) is a key determinant of future fracture risk. If there are deficits in adolescent bone acquisition they are likely to be permanent leading to increased fracture risk in adult life. Thus, impaired bone metabolism in adolescents with morbid obesity could have a long-standing impact on bone health and fracture risk in this younger population.”
“Obesity does not protect against bone loss as previously thought; it is important to promote bone health in adolescents with obesity through diet and exercise. Obesity was always thought to be protective for bone but we show that increased visceral fat mass (the deep belly fat that surrounds our organs) and total fat mass have negative effects on cortical bone.”
“This was a pilot study in adolescents with morbid obesity who will undergo weight loss surgery (bariatric surgery). We will examine the same adolescents one and two years after weight loss surgery to assess the effect of such surgery on bone.”
Education Improves Knee Replacement
An educational video might make a big difference when it comes to reducing racial variations in health care utilization and outcomes. The researchers, who hail from the University of Pennsylvania (Penn) Perelman School of Medicine, randomly assigned 336 study participants to either see the video describing the surgical risks and benefits, or receive an educational booklet. All 336 of the participants self-identified as Black, were 50 years or older with chronic and frequent knee pain, and exhibited radiographic evidence of OA.
Said A. Ibrahim, M.D., M.P.H., M.B.A. of the Penn Perelman School of Medicine, told OTW, “This is part of our effort to address racial variations in health care utilization and outcomes. We began this work by first documenting racial disparity in joint replacement utilization rates. We then conducted studies to understand the reasons for this particular disparity. We identified patient preference for surgery as one of the most important factors in this disparity. We then conducted studies to examine how to best address racial variation in preference rates for joint replacement. In the past we reported on the effectiveness of a knee decision aid in improving minority patients’ preferences and knowledge regarding joint replacement. This study was designed to show whether a knee osteoarthritis (OA) decision aid actually impacts surgical rate, not just patient preference.”
“The most important message for orthopedic surgeons is that minority patients are open to surgery provided they are educated about the risks/benefits of joint replacement. Given how busy orthopedic surgeons are, it is unlikely they will have the time needed to fully educate patients about joint replacement. Therefore, decision aids are a reasonable alternative to extensive doctor-patient discussions about surgery.”
“We were surprised by the size of the treatment effect. We hypothesized that the surgery rate would go up among patients who viewed the decision aid video, but not by 85% (compared to those who did not view the decision aid video). This finding needs to be replicated.”
“We are planning to conduct an effectiveness-implementation hybrid type I study to a) replicate the findings of this study by including orthopedic patients in other cities such as Houston and Baltimore, b) to assess implementation data that would facilitate widespread availability and use of knee decision aids in orthopedic practices where large number of minority patients receive care. Lastly, we are testing whether the effect we found in African-American patients is also present among White patients of similar clinical and socioeconomic background.”
Avoiding Tunnel Convergence in Knee Surgery
A descriptive laboratory study undertaken by the Steadman Philippon Research Institute and the Oslo University Hospital/University of Oslo has resulted in new information on managing torn knee ligaments. The researchers set out to assess the risk of tunnel convergence in multiple ligament reconstructions and determine the best tunnel placement for the reconstruction of multiple ligaments in the tibia.
Robert F. LaPrade, M.D., Ph.D., is chief medical officer and co-director of the Steadman Philippon Research Institute. He commented to OTW, “This was a collaborative work between Gilbert Moatshe, M.D. (the first author) and Lars Engebretsen, M.D., Ph.D. at the Oslo University Hospital/University of Oslo and the Steadman Philippon Research Institute. Tunnel convergence is one of the hot topics in orthopedic meetings among surgeons treating complex knee injuries. Biomechanical and clinical studies have demonstrated that anatomic reconstruction provides improved outcomes. However, during multiligament reconstructions there is a limited bone stock to accommodate all the tunnels. We wanted to evaluate the risk of tunnel convergence and come up with some guidelines of how to avoid convergence to help surgeons treating these complex injuries. This is particularly important for young surgeons treating these injuries especially and those with limited volume.”
“We developed 3D knee models using computed tomography images of 21 patients; then software was used to create tunnels for each of the four primary ligamentous structures. We found a high risk of tunnel convergence (66.7%) between the posterior cruciate ligament (PCL) and posterior oblique ligament (POL) tunnels when the POL tunnel was aimed toward the Gerdy’s tubercle (as suggested in the literature). There was no tunnel convergence when the POL tunnel was aimed 15 mm medial to the Gerdy tubercle; no tunnel convergence was observed between the anterior cruciate ligament (ACL) and POL. Tunnel convergence was observed between the PCL and superficial medial collateral ligament (sMCL) in 19.0% of cases when the sMCL tunnel was aimed transversely across the tibia.”
“There is a high risk of tunnel convergence during multiligament knee reconstructions. With proper planning of the surgery, tunnel placement and orientation, biomechanically and clinically validated anatomic reconstructions can be safely performed.”
“The most interesting finding was that despite the limited bone stock on the distal femur, tunnel convergence can be avoided by good surgical planning. Double bundle PCL reconstruction has demonstrated to better restore knee stability than single bundle PCL reconstructions. However, some surgeons prefer to perform single bundle PCL reconstructions in multiple ligament reconstructions because of the concern for potential tunnel convergence. The study demonstrates that anatomic double bundle PCL can safely be performed in multiligament injuries. In addition, anatomic posterolateral corner reconstructions can be safely performed concurrently with ACL reconstructions.”
“One of the main questions in complex knee injuries is how the tensioning sequence of the reconstruction ligaments affects the knee joint kinematics and hence both short term and long term outcomes. Our next project is to use the results from this study to investigate the biomechanical consequences of the tensioning sequence on knee kinematics and hopefully the graft tensioning sequence that restores the native knee kinematics.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.