Johns Hopkins researchers have found a bacterium that causes chronic inflammatory gum infections also triggers the inflammatory autoimmune response characteristic of rheumatoid arthritis (RA).
Gum Bacterium Triggers RA Response
3 min read Premium comments
Secondary
“This is like putting together the last few pieces of a complicated jigsaw puzzle that has been worked on for many years, ” said Felipe Andrade, M.D., Ph.D., in the December 14, 2016 news release. Dr. Andrade, the senior study investigator and associate professor of Medicine at the Johns Hopkins University School of Medicine, also practices at Johns Hopkins Bayview Medical Center.
First author Maximilian Konig, M.D., a former Johns Hopkins University School of Medicine fellow now at Massachusetts General Hospital, told OTW, “The idea that RA, although an autoimmune disease, may be initiated by a microbial infection is not novel, but has been speculated on for more than a century. One intriguing clinical observation is the fact that patients with RA frequently have severe periodontal disease and that some patients with periodontal disease may be at increased risk of developing RA. However, our limited understanding of the disease mechanisms that drive and sustain the autoimmune response in RA made it impossible to pinpoint a specific bacterial trigger.”
“In recent years, our understanding of the abnormal immune response in RA has grown exponentially, and we now know that disease-specific autoantibodies (ACPAs) target and attack post-translationally modified proteins (this modification is known as citrullination) and that this abnormal immune response to citrullinated proteins appears to drive the joint inflammation and destruction seen in RA.”
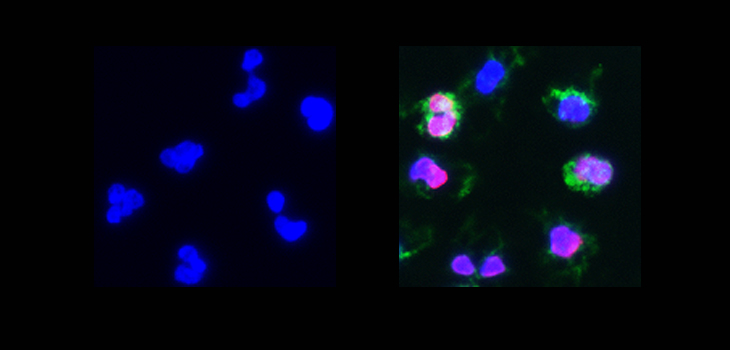
“Recent studies from our laboratory at Johns Hopkins that were led by Felipe Andrade, M.D., Ph.D. suggested that neutrophils appear to be the source of many citrullinated proteins targeted in this disease, and we identified a process called leukotoxic hypercitrullination in neutrophils which is driven by immune pathways that create pores in the neutrophil membrane, thereby activating the cell to generate autoantigens. These autoantibodies are known as anti-citrullinated protein antibodies (ACPAs) and are frequently measured clinically using the CCP [cyclic citrullinated peptides] assay.”
“We showed that the periodontal pocket in patients that are infected with the periodontal pathogen Aa [Actinobacillus actinomycetemcomitans] mimics the rheumatoid joint—in that they harbor the same citrullinated autoantigens targeted by ACPAs in patients with RA. We then realized that the mechanism by which Aa drives the generation of RA autoantigens was very similar to what we had seen before in the inflamed joints of patients with RA: Aa produces a pore-forming toxin that specifically binds to neutrophils in the periodontium and induces leukotoxic hypercitrullination in neutrophils that subsequently die and release citrullinated proteins into the extracellular space.”
“In our study, almost 50% of patients with RA had evidence of Aa infection (as compared to 11% of healthy controls). The strongest previously identified genetic risk factor for ACPA production and RA, HLA-DRB1 shared epitope alleles, only conveys this risk if the patient has also been infected with Aa. It appears you need both, the right genetic background to present citrullinated proteins to the immune system and an infection that drives the production of abnormal citrullinated proteins (such as Aa) to develop disease-specific antibodies and possibly RA.”
“At this point, how these findings are best applied to patients with RA remains uncertain. However, it opens the possibility of primary prevention in patients at risk as RA often takes years to develop. In this phase of the disease, patients already have autoantibodies, but remain asymptomatic or minimally symptomatic. It will also be fascinating to see what happens when we target the bacterium directly in infected patients that have established RA.”
For more information on this study (Konig MF et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Science Translational Medicine, 14 Dec 2016: Vol. 8, Issue 369, pp. 369ra176. DOI: 10.1126/scitranslmed.aaj1921), please visit the web site at http://stm.sciencemag.org/content/8/369/369ra176.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.