The results of a controlled laboratory study from Mayo Clinic are shedding light on the complexity of non-contact anterior cruciate ligament (ACL) injuries. The research, recently published in the American Journal of Sports Medicine, involved a cadaveric model of landing. According to the study, “Peak ACL strain was measured in situ and characterized under impulsive axial compression and simulated muscle forces (baseline) followed by addition of anterior tibial shear, knee abduction, and internal tibial rotation loads in both uni- and multiplanar modes, simulating a broad range of landing conditions. The associations between knee rotational kinematics and peak ACL strain levels were further investigated to determine the potential noncontact injury mechanism.”
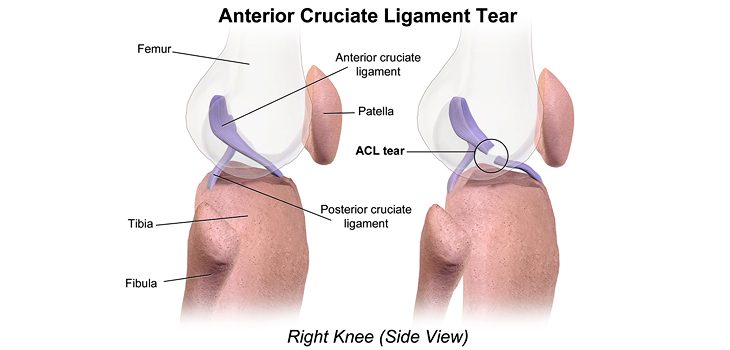
Non-Contact ACL Injuries: Prevention Needed!
Timothy E. Hewett, Ph.D., is a study author who is with the department of Physiology & Biomedical Engineering at Mayo Clinic in Rochester, Minnesota. He told OTW, “Over two-thirds of ACL ruptures occur via non-contact mechanisms during landing and there is a 2-10 fold greater incidence in females compared to males. The greatest ACL strains occur with a combination of rotations and loads in all 3 planes of motion—knee abduction, lateral compartment anterior shear and internal tibial rotation!
“Prevention programs, rehabilitation protocols and surgical techniques that decrease this combination of rotations and loads in all three planes of motion—knee abduction, lateral compartment anterior shear and internal tibial rotation—will decrease strain on the ACL and reduce risk of first or second ACL injury.
“If athletes after an ACL reconstruction are young, active and return to the same level of sports, their risk of a second ACL tear via these mechanisms of combined rotations and loads in all three planes of motion are between a quarter (25%) and a third (35%)!”
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.