Daniel C. Allison, M.D., a board-certified orthopedic surgeon in Los Angeles, is preparing to perform the first bone anchored (osteointegrated) prosthesis surgery to be done in Southern California. The patient had previously had an above-the-knee-amputation.
First Osteointegrated Surgery Performed in California
1 min read Premium comments
Secondary
“We are very excited to be the first practice in Southern California to offer the surgery, ” said Allison. “We are constantly working to bring the latest surgical innovation techniques to our joint replacement and hip arthroplasty treatments.”
Surgeons installing traditional prosthetics use a ball and socket design. The socket is placed around the end of the affected limb, to which the prosthetic arm or leg is then attached. This approach requires enough surface area on the remaining limb to adequately attach the cap with the socket. It can also present issues with comfort and fit, according to the September 18, 2016 PRWeb press release.
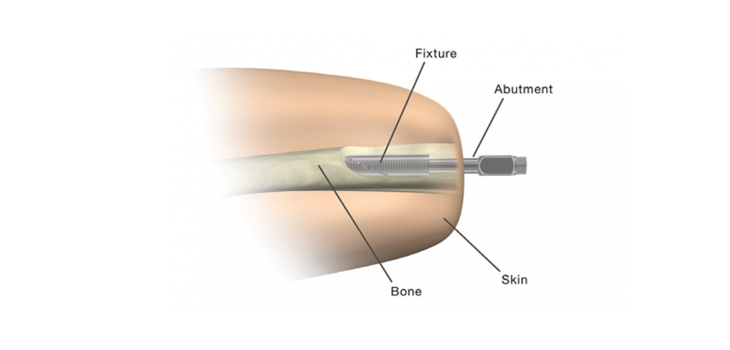
In making use of the Osseoanchored Prosthesis for the Rehabilitation of Amputees (OPRA), manufactured by Integrum AB in Molndal, Sweden, surgeons implant a titanium fixture directly into the bone. Using a titanium implant, they say, helps to mitigate the risk of rejection from the bone. Once the fixture has integrated and healed, surgeons attach a rod through the skin, which then connects to the prosthetic leg. The benefits of this approach include greater mobility, range of motion, and comfort. It also offers hope for amputees who are not good candidates for or have had limited success with traditional socket prosthetics.
The OPRA prosthesis has been approved by the FDA (Food and Drug Administration) for use in above the knee amputees. “With proper care and comprehensive physical therapy and rehabilitation, we are very optimistic that this approach will offer a significant improvement in quality of life for many adults, especially veterans with above-the-knee amputations, ” said Allison.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.