A new study suggests that osteoporosis patients are not getting the care they need.
“Crisis” as High Risk Fracture Patients Go Undiagnosed, Untreated
2 min read Premium comments
Secondary
According to the June 23, 2016 news release, Sundeep Khosla, M.D., a practicing endocrinologist, research scientist, professor of medicine and director of the Clinical and Translational Science Award Program at the Mayo Clinic in Rochester, Minnesota, and Elizabeth Shane, M.D., a practicing endocrinologist, research scientist, professor of medicine and vice chair for clinical and epidemiological research at Columbia University have found too many patients at high risk for fractures are not being diagnosed or treated to prevent them.
The authors state, “We should be viewing the future for our patients with osteoporosis with unparalleled optimism, because we now have several drugs that can markedly reduce fracture incidence, by as much as 70% in the case of vertebral fractures. Thus, while physicians still struggle to treat many other conditions that are currently intractable, including Alzheimer’s and many cancers, the good news is that the prevention of fractures is clearly within our reach. And yet, despite the development of several effective drugs to prevent fractures, many patients, even those who unequivocally need treatment, are either not being prescribed osteoporosis medications at all, or when prescribed, refuse to take them.”
Asked what gets in the way of a physician prescribing these drugs, Dr. Khosla told OTW, “Osteoporosis may be one of multiple conditions the patient has (e.g., diabetes, heart failure) and the physician just does not give it sufficient priority. Sometimes, there is just a lack of physician awareness about the disease. More recently, concerns about the relatively rare side effects of bisphosphonates (i.e., osteonecrosis of the jaw, atypical femur fractures).
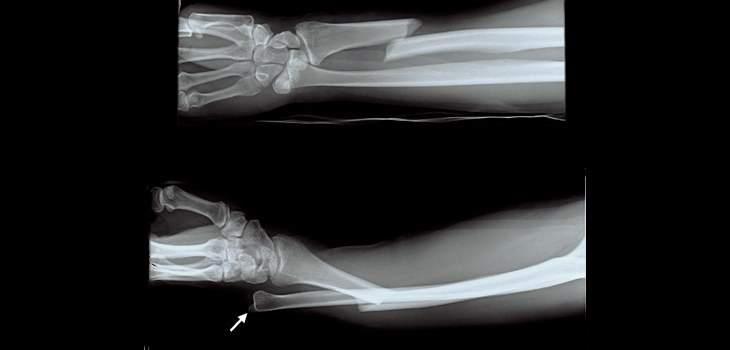
“A patient who has had an osteoporotic fracture (e.g., of the distal radius, spine, hip, or upper arm) is at increased risk of subsequent fracture and is generally a candidate for pharmacological therapy. Any patient over 50 years of age who has one of these fractures should have a DXA [dual X-ray absorptiometry] bone density scan and be considered for treatment.
“We clearly need better ways to proactively identify the rare group of patients who develop osteonecrosis of the jaw or atypical femur fractures. Fear of these complications is keeping many patients who could truly benefit from these drugs from taking them.”
Asked what more can be done, Dr. Khosla noted, “Better patient and physician education about the consequences of untreated osteoporosis—disability, pain, and increased mortality following hip fracture. Also, more work on educating patients in particular about the benefit to risk ratio of bisphosphonates and other osteoporosis drugs. For a patient meeting current guidelines for treatment, considerable data shows that the benefits far outweigh the risks and that the risks from a hip fracture far outweigh the rare risks from the treatments. But we still need to work on identifying the patients at risk for complications from these medications.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.