New work involving 503 athletes has found that sex, age, and graft size matter when it comes to an ACL (anterior cruciate ligament) re-tear post reconstruction with a hamstring graft. The research, led by Duong Nguyen, M.D. has just been presented at the American Orthopaedic Society of Sports Medicine’s Annual Meeting in Colorado Springs, Colorado. Dr. Nguyen and his team studied a cohort of athletes undergoing primary, autograft hamstring ACL reconstruction.
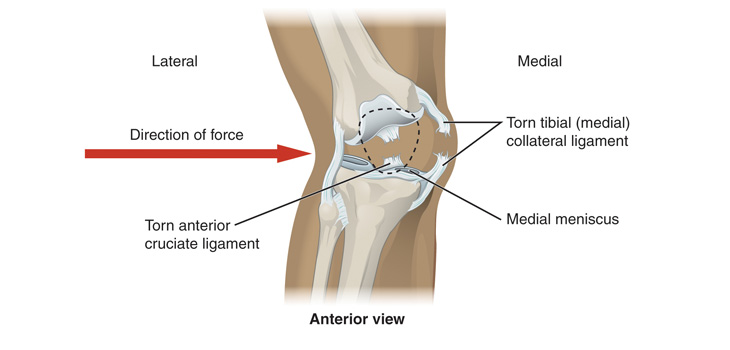
ACL: Increased Risk for Young Female Patients
2 min read Premium comments
Secondary
“Our research noted that female patients under the age of 25 with a graft size of less than 8 mm have an increased chance of re-tearing their ACL following reconstruction. Another contributing issue to this increased re-tear rate might also be due to pre-disposing factors, including estrogen levels, anatomical differences, and decreased knee strength. More research is needed to further determine the exact causes, ” said Dr. Nguyen in the July 7, 2016 news release.
As indicated in the news release, “The surgeries were all performed at a single center by a single surgeon between September–December 2012 and were followed for a duration of two years. The average age of the athletes was 27 with 235 females and 268 males taking part in the study. The same surgical technique was used during all of the procedures. Patients were allowed to return to sports participation between six and 12 months post-surgery only if they were pain-free, had equal quadriceps/hamstring strength and if they had graduated from the rehabilitation program.”
“Given the results of our study, we feel that surgeons should counsel their younger, female patients accordingly and consider modifying their surgical techniques to utilize larger size grafts and/or rehabilitation strategies to lessen the chance of a re-tear, ” said Dr. Nguyen.
Dr. Nguyen told OTW, “We suspected these three factors would contribute to the risk of ACL re-tear. We were just surprised to learn the magnitude of the effect.”
“ACL re-tear is multifactorial and surgeons should consider other potential causes such as the specific sport played, the athlete’s level of competition and position on the team, the extent of contact in the sports activity, and the patient’s tendency for risk taking behavior which are harder to quantify and control in a study.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.