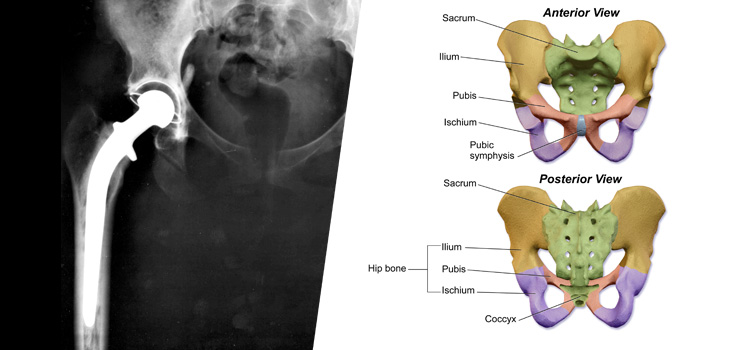
The verdict is in…surgical approach to total hip replacement (THR) has no impact on outcomes six months after surgery. There is no difference if you go in from the front of the body or the side/back (anterior versus posterior).
Anterior, Posterior: It’s all the Same for THR
1 min read Premium comments
Secondary
According to the March 3, 2016 news release, the new research, conducted at Saint Francis Hospital & Medical Center in Hartford, Connecticut, involved 274 patients who underwent THR between June 2012 and August 2014. Patients had the procedure with a surgeon either exclusively performing a direct anterior approach, or a surgeon exclusively performing a posterior approach. The two groups were compared on pre- and post-surgical pain, other symptoms, function in daily living, function in sports and recreation, and hip-related quality of life.
“Both direct anterior and posterior surgical approaches for THR yield excellent, equivalent results as reported by patients, ” said lead study author Mike Cremins, Ph.D., PA-C. “The surgical approach alone is not the singular variable that yields a difference in six-month postoperative outcome.”
“Patients considering THR should ask their orthopedic surgeon about the surgeon’s surgical approach experience and preference, ” said co-author and orthopedic surgeon John Grady-Benson, M.D. “A preoperative shared decision-making discussion should always incorporate risks and potential benefits of any surgical approach to THR, as well as help patients understand what they can do before and after surgery to optimize outcomes.”
Dr. Cremins told OTW, “The controversy is simply that the existing data is confusing. There are an equal number of papers for each approach claiming superiority. Surgeons have considered changing their preferred surgical approach because of this.”
“We were interested in this topic because we have a large number of surgeries performed with each approach and we wanted to see from the patients perspective which was superior.”
“The message to orthopedic surgeons is choose one surgical approach and master it. Make sure your surgical team masters it as well. If so, your patients will do well regardless of the approach you perform.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.