Comprehensive Study Looks at Early Osteolysis in TAA
Osteolysis in Total Ankle Arthroplasty: Why So Many Early Failures? // Stunning New Implant Data From Registry Consortium // and More!
7 min read Premium comments
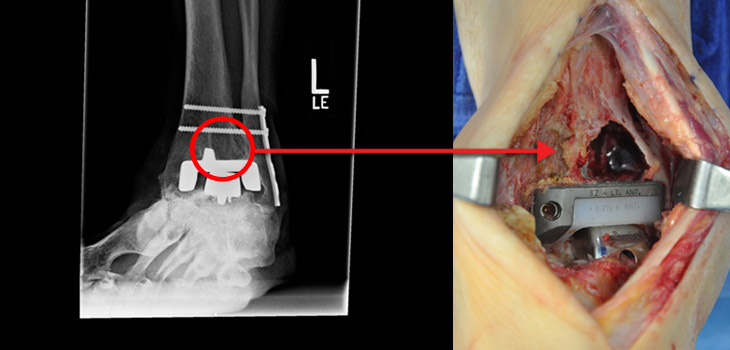
Why are foot and ankle specialists seeing early osteolysis of their total ankle arthroplasties (TAA)? Steven Haddad, M.D., immediate past president of the American Orthopaedic Foot and Ankle Society (AOFAS), wants to figure it out. Dr. Haddad, an orthopedic surgeon with Illinois Bone and Joint Institute, LLC, told OTW, “Many of my foot and ankle colleagues are seeing patients who have undergone TAA show up with osteolysis as early as three years following surgery; some estimates run as high as 15% within that timeframe. This is in stark contrast to hip and knee surgery, where osteolysis typically occurs much later.”
“Our team competed for a grant from the Orthopaedic Research and Education Foundation (OREF), and we were awarded $100, 000 to study this issue. Our goal is to assess polyethylene particle wear after TAA as a potential cause of osteolysis that leads to early failure. Although we assume that polyethylene disease is the culprit, recent Finnish studies have biopsied specimens from prostheses generating substantial osteolysis, and found no polyethylene wear particles in those samples. These authors feel that osteolysis in TAA occurs from a different source: necrosis of bone around the implant stimulating the RANKL (receptor activator of nuclear factor kappa-B ligand) pathway. It is our goal to provide a comprehensive assessment to either confirm or deny this conjecture. We wish to know whether the pathway to osteolysis occurs due to polyethylene wear, or some other currently undefined mechanism.”
“Our team proposed an aggressive, multifactorial study where we perform both a macro and micro evaluation. We will be testing three different ankle prostheses through five million cycles (each brand of prosthesis will undergo three testing cycles). We will be comparing the volumetric and linear wear rates of each polyethylene component in each prosthesis. In addition, we will be evaluating tissue samples obtained from over one hundred patients with osteolysis following TAA (from a variety of implants). We anticipate that combining this data will give substantial insight as to the biomechanics involved in generating osteolysis.”
“Our goal is to use this combined data as a springboard to understand the role of total ankle implant design in potentially generating earlier osteolysis than seen by our hip and knee colleagues. We hope to combine newer technology where fluoroscopy and gait analysis are used to understand how different ankle implants articulate in vivo. We can then extrapolate this data to perform secondary wear testing on these same three total ankle prostheses, comparing this to the data we obtain through standard methodology in our index analysis. This type of ‘anatomic motion’ wear testing is currently being explored for total knee components, giving us the most complete understanding of osteolysis generation.”
“This research is critical because TAA is exploding in popularity amongst surgeons. It is an escalating procedure in managing end stage ankle arthritis, while fusion rates remain flat. Our goal is to persevere in studying this last variable element in predictability of prosthesis longevity. With this knowledge, we hope to equal our hip and knee colleagues in improving upon long-term successful total ankle arthroplasty outcomes for our patients.”
International Orthopedic Registry Consortium Employs Advanced Algorithms to Reveal Hidden Implant Data. Clue: Mobile Non-PS Bearings May Not Be Great Option
The International Consortium of Orthopedic Registries (ICOR) has exploded on the scene in recent years as a serious, thorough research endeavor. And they are getting some pretty interesting results. Art Sedrakyan, M.D., Ph.D., Sc.D. is the principal investigator of this FDA funded project. He told OTW, “With ICOR, we are seeing what 21st century surveillance might start to look like, namely, literature reviews, primary data collection, and working with clinician leaders worldwide for multi-national investigations. We developed an algorithm that allows us to combine summary data. That is summary level information obtained from each country/registry in a harmonized fashion…data is stratified by age, distribution of cement use, head sizes, etc. You can combine this harmonized information in a similar way from each participating registry.”
Asked about recent ICOR results, Dr. Sedrakyan noted, “The most interesting findings are those involving the hip bearings, mobile knee and posterior stabilized knee implants. For example, we compared fixed with mobile knees and found that the mobile bearings had worse outcomes than fixed bearings. Because we were looking at specific causes of revisions we can’t tell why, but there was, in fact, a substantially higher risk of revision associated with mobile bearings…and, this is a long-term follow-up study.”
“I think orthopedic surgeons need to take note and think about possible reasons for this. Within ICOR we are taking a patient-centered approach and looking at all cause revision. Despite these studies not yet receiving much attention, in my opinion these are groundbreaking findings not reported before. Some estimates indicate that 30% of the bearings implanted annually might be mobile bearings. We need to understand why these failures occur and communicate this to the FDA. If patients ask for a mobile device seeking more functionality they have to be aware of the risk. Moreover, based on our systematic reviews they might not necessarily be getting that additional functionality. Many surgeons believe that these bearings are completely similar in terms of long-terms outcomes. Our hope is that this work will reach the average practicing orthopedic surgeons so that their patients can benefit from internationally accumulated knowledge.”
“On another note, we just had the annual meeting of Medical Device Epidemiology Network at FDA and discussed implementation of UDI (Unique Device Implementation) program for future surveillance of devices such as hip and knee implants. This will be extremely useful in tracking devices throughout their lifetimes. Unfortunately, major payers such as Medicare are not interested in implementing UDI even for implants within claims data due to logistics and expenses. In addition, there are two additional problems that we are facing. First, even if UDI is implemented we need a way to easily extract this from claims data and link it to clinical data in order to study and classify it. Second, we need to better understand long-term outcomes. How do you follow up with people? The only way to know is if we link to other claims (insurance, payor, or Medicare claims) and see if long-term outcomes such as revision occurs. But claims data sources are not well integrated, and the longitudinal data is limited.”
“We have just received a new grant to create a network of U.S. registries that will allow us to explore linking to claims. It is a demonstration project that will hopefully soon become a coordinated registry network based on orthopedic registry data, claims from data owners and other stakeholders.”
Psychiatric Dx Greatly Increases Complications, Discharge to Inpatient Facility
Depression, anxiety, dementia and schizophrenia…one or more of these issues are faced by some orthopedic patients at one time or another—and these psychiatric comorbidities can very well affect your surgical outcomes. Wael Barsoum, M.D., president of Cleveland Clinic, Florida, always suspected that orthopedic surgeons were undertreating patients with psychiatric disorders. Dr. Barsoum, who has overseen a 17-year analysis of 8.3 million patients, tells OTW, “There are few studies in orthopedics that examine these issues and the roles they may play in a patient’s recovery, but the reality is that orthopedic surgeons encounter troubled patients on a daily basis. With risk sharing and bundled payments becoming the status quo in the current healthcare climate, understanding how these comorbidities play a role in the overall treatment picture is essential.”
“We can predict which patients should receive treatment, if he or she is not already, for psychiatric problems before undergoing surgery. Many of these patients are likely treatable preoperatively; if we can get them the appropriate treatment, their chances for better physical outcomes are enhanced. If the cost to treat these patients is substantially high due to increased adverse events and poorer outcomes, some hospitals and doctors will refuse to treat them. If the hospital is getting a fixed amount of money due to a bundled payment system, they are likely to tell patients, ‘Go to a tertiary care center.’”
“Our findings show that if a patient has schizophrenia—even if treated preoperatively—their risk of an adverse event is 56% higher than a patient who does not have this condition. For someone who is depressed the risk of complications is 20% higher than someone who is not depressed. Interestingly, schizophrenia and depression predict the need for blood transfusions. While we don’t have any definitive answers as to why this is, patients with these conditions often report fatigue, which mimics anemia.”
“Discharge to an inpatient facility is a substantially higher cost that a routine discharge home. With that in mind, consider the increased costs involved with patients with dementia, who were 4.5 times more likely to require discharge to an inpatient facility than patients without that diagnosis. Patients with schizophrenia had a 2.4 times higher chance of requiring this kind of discharge, while for those diagnosed with depression the risk was 1.1 times higher than those without depression. This information is critical in determining how we can best partner with our psychiatric colleagues to optimize care for these patients. Organ transplant patients and bariatric surgery patients routinely undergo a psychiatric exam prior to surgery. I am not suggesting that every orthopaedic patient needs a psychiatric evaluation. However, if an orthopedic surgeon finds yellow/red flags in the psychiatric history of a patient, he or she should have a psychiatric exam administered to that patient preoperatively.”
“As we are now in a period of healthcare reform and risk sharing, it is more imperative than ever that we are willing to undertake appropriate risk stratification. If you have a patient who is 92 with a history of renal failure, for example, then you know that the cost will be greater than doing hip replacement on a healthy 62 year old with arthritis. The issues we face are no different in terms of mental health. A better understanding of the increased risk is needed to first, ensure that the patient is preoperatively optimized, and second, create appropriate bundled care strategies.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.