Vanderbilt researchers are shaking things up in the world of fracture care. The scientists have discovered that contrary to popular belief, fibrin is not required for fracture healing. Instead, fibrin breakdown must happen in order to have healthy fracture repair.
Fibrin Not Necessary for Fracture Healing?!
2 min read Premium comments
Secondary
“Many of the current pharmaceutical protocols are based on using fibrin to promote fracture healing, ” said Jonathan Schoenecker, M.D., Ph.D., assistant professor of Orthopaedic Surgery and Rehabilitation, in the August 11, 2015 news release. “In certain instances it may help, but we’ve shown for sure that you don’t need it. Bone biology does not require fibrin to heal a fracture.”
It was previously thought that fibrin promoted repair by providing a scaffold for the initial phase of new bone formation. But the Vanderbilt team found that fracture repair was normal in mice missing the fibrin precursor fibrinogen.
“Fibrin puts a cog in the machine and you don’t get the anastomosis (vessel reconnection), ” Schoenecker said.
The findings may explain why obesity, diabetes, smoking and advanced age impair fracture repair. They are all associated with impaired fibrin clearance, he explained. The investigators also found that mice unable to clear fibrin formed bone in muscle (heterotopic ossification).
Dr. Schoenecker told OTW, “Now that we have identified that the removal of fibrin is essential to heal fractures any pharmacologic with the capacity [to] reduce the amount of fibrin deposited in a fracture or promote its removal may function to enhance fracture healing. The big trick to developing these pharmaceuticals for orthopaedics is to optimize their ability to improve fracture healing without compromising fibrin’s principle role—to stop a patient from bleeding. Currently, we are in preclinical animal trials with promising results.”
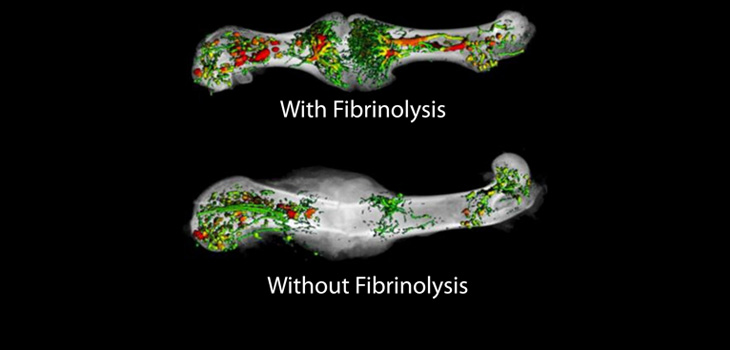
“In order to figure out how fibrin blocks fracture healing, we had to first figure out exactly how a fractured bone re-establishes its blood supply. To do so we started from the published models on this topic and took a big leap forward by developing a new technique allow for visualization of new bone and blood vessels at the same time. From this data we proposed an entirely new model of the process of fracture revascularization. Most importantly, we learned that fractures heal by first shunting blood flow from the inside of the bone to outside the bone. Then blood vessels grow outside the bone and connect to each other from opposite ends. This new model emphasizes the importance of the anatomic location of these newly developing vessels providing insight into how a device, such as an intramedullary nail on the inside of the bone or a plate on the outside of the bone, would impede or help this vascular process. From this information we are working on devices that stabilize the fracture, but do not get in the way of this essential process. Together, our findings strongly suggest the optimal treatment for fracture healing is a device that does not disrupt revascularization of a fracture and pharmacologics that limit or promote fibrin in the fracture bed.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.